

Value of accurate diagnosis for metastatic supraclavicular lymph nodes in breast cancer: assessment with neck US, CT, and 18F-FDG PET/CT
- PMID: 34003120
- PMCID: PMC8136540
- DOI: 10.5152/dir.2021.20190
Value of accurate diagnosis for metastatic supraclavicular lymph nodes in breast cancer: assessment with neck US, CT, and 18F-FDG PET/CT
Abstract
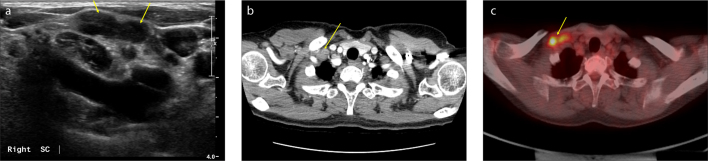
Purpose: Neck ultrasonography (US), computed tomography (CT), and 18F-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) are all known to be useful imaging modalities for detecting supraclavicular lymph node (SCN) metastasis in breast cancer. The authors compared the diagnostic values of neck US, CT, and PET/CT in the detection of SCN metastasis in breast cancer.
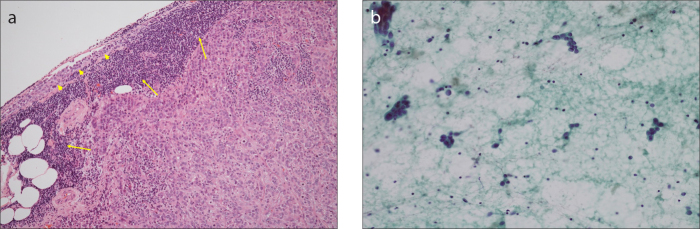
Methods: SCN metastases identified in neck US, CT, or PET/CT during follow-up visits of patients with breast cancer were pathologically confirmed with the use of US-guided fine-needle aspiration cytology. The clinicopathological factors of the patients were analyzed, and the statistical parameters including sensitivity, specificity, positive and negative predictive values, false-positive and false-negative rates, and accuracy of neck US, CT, and PET/CT were compared.
Results: Among 32 cases of suspicious SCNs, 24 were pathologically confirmed as metastasis of breast cancer. The sensitivity of US + CT was 91.7%, which was the same as that of PET/CT, while the sensitivity rates of US alone and CT alone were 87.5% and 83.3%, respectively. Accuracy was 99.8% in PET/CT alone and 98.1% in US + CT. The false-negative rate was 0.1% in US + PET/CT, while it was 0.2% in PET/CT and US + CT, 0.3% in US alone and 0.4% in CT alone.
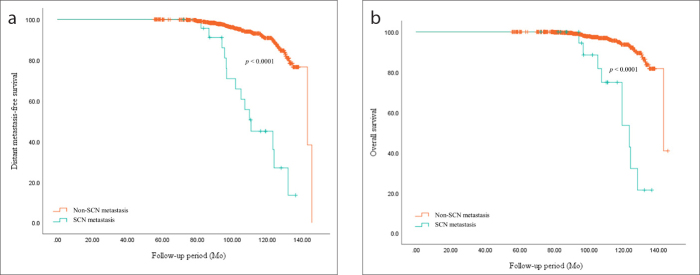
Conclusion: PET/CT can be the first choice for detecting SCN metastases in breast cancer. However, if PET/CT is unavailable for any reason, US + CT could be a good second option to avoid false-negative results.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
-
- Narod SAIJ, Miller AB. Why have breast cancer mortality rates declined? J Cancer Policy. 2015;5:8–17. doi: 10.1016/j.jcpo.2015.03.002. - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
