

Association of Coronary Artery Bypass Grafting vs Percutaneous Coronary Intervention With Memory Decline in Older Adults Undergoing Coronary Revascularization
- PMID: 34003225
- PMCID: PMC8132142
- DOI: 10.1001/jama.2021.5150
Association of Coronary Artery Bypass Grafting vs Percutaneous Coronary Intervention With Memory Decline in Older Adults Undergoing Coronary Revascularization
Abstract
Importance: It is uncertain whether coronary artery bypass grafting (CABG) is associated with cognitive decline in older adults compared with a nonsurgical method of coronary revascularization (percutaneous coronary intervention [PCI]).
Objective: To compare the change in the rate of memory decline after CABG vs PCI.
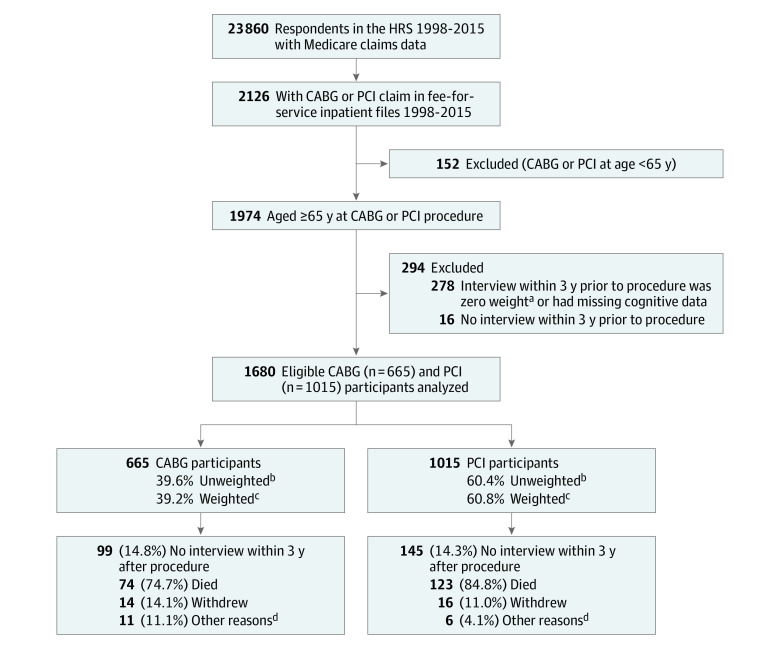
Design, setting, and participants: Retrospective cohort study of community-dwelling participants in the Health and Retirement Study, who underwent CABG or PCI between 1998 and 2015 at age 65 years or older. Data were modeled for up to 5 years preceding and 10 years following revascularization or until death, drop out, or the 2016-2017 interview wave. The date of final follow-up was November 2017.
Exposures: CABG (including on and off pump) or PCI, ascertained from Medicare fee-for-service billing records.
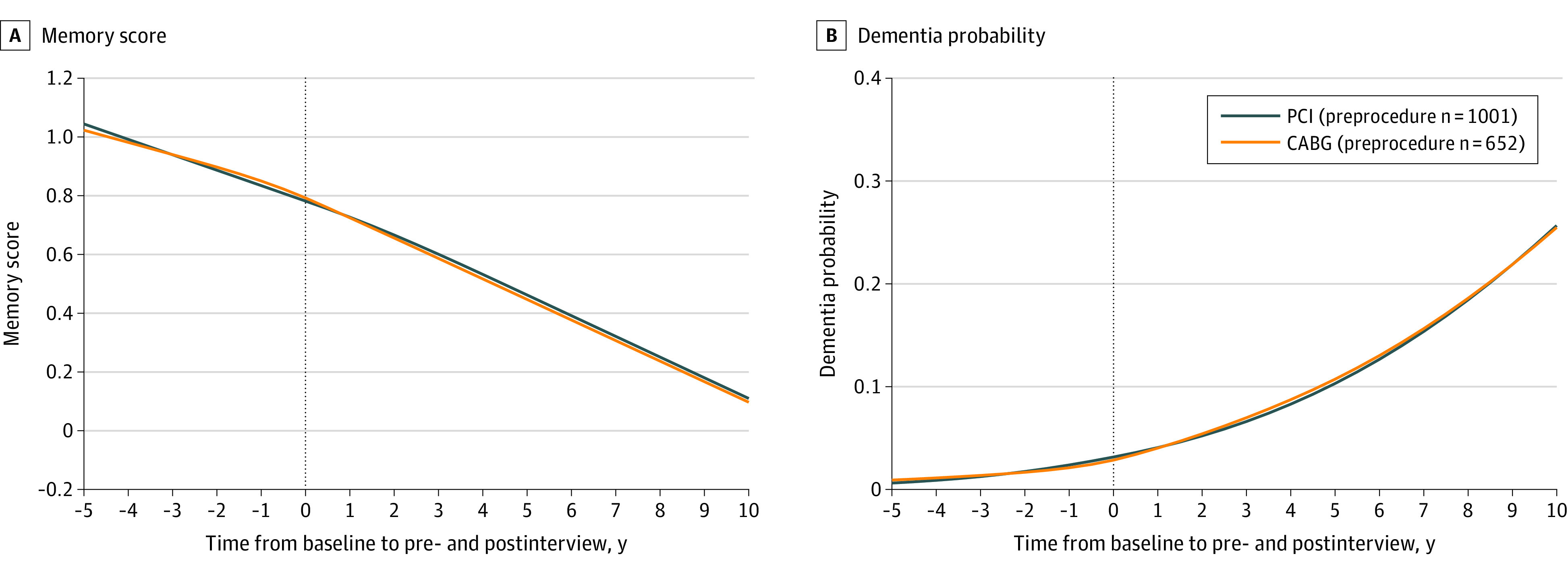
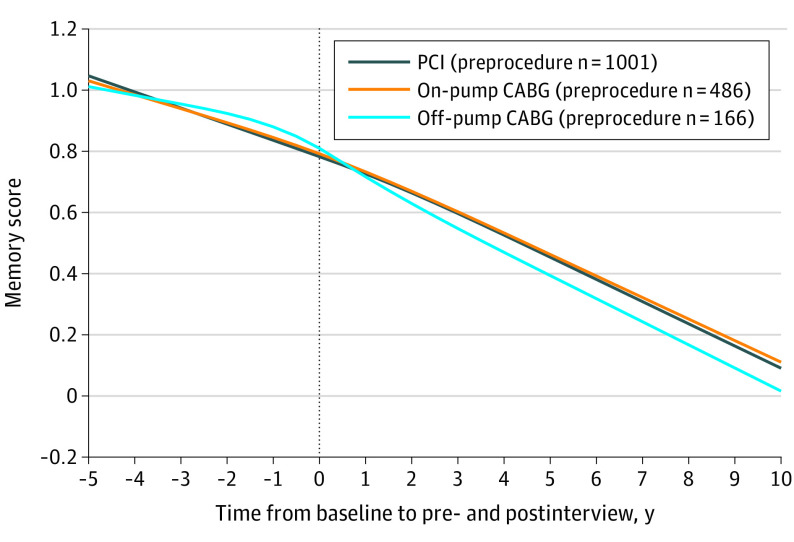
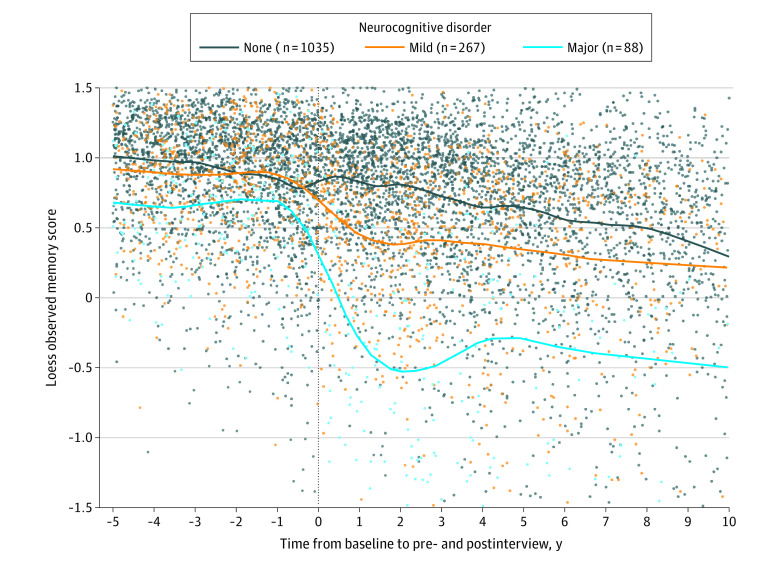
Main outcomes and measures: The primary outcome was a summary measure of cognitive test scores and proxy cognition reports that were performed biennially in the Health and Retirement Study, referred to as memory score, normalized as a z score (ie, mean of 0, SD of 1 in a reference population of adults aged ≥72 years). Memory score was analyzed using multivariable linear mixed-effects models, with a prespecified subgroup analysis of on-pump and off-pump CABG. The minimum clinically important difference was a change of 1 SD of the population-level rate of memory decline (0.048 memory units/y).
Results: Of 1680 participants (mean age at procedure, 75 years; 41% female), 665 underwent CABG (168 off pump) and 1015 underwent PCI. In the PCI group, the mean rate of memory decline was 0.064 memory units/y (95% CI, 0.052 to 0.078) before the procedure and 0.060 memory units/y (95% CI, 0.048 to 0.071) after the procedure (within-group change, 0.004 memory units/y [95% CI, -0.010 to 0.018]). In the CABG group, the mean rate of memory decline was 0.049 memory units/y (95% CI, 0.033 to 0.065) before the procedure and 0.059 memory units/y (95% CI, 0.047 to 0.072) after the procedure (within-group change, -0.011 memory units/y [95% CI, -0.029 to 0.008]). The between-group difference-in-differences estimate for memory decline for PCI vs CABG was 0.015 memory units/y (95% CI, -0.008 to 0.038; P = .21). There was statistically significant increase in the rate of memory decline after off-pump CABG compared with after PCI (difference-in-differences: mean increase in the rate of decline of 0.046 memory units/y [95% CI, 0.008 to 0.084] after off-pump CABG), but not after on-pump CABG compared with PCI (difference-in-differences: mean slowing of decline of 0.003 memory units/y [95% CI, -0.024 to 0.031] after on-pump CABG).
Conclusions and relevance: Among older adults undergoing coronary revascularization with CABG or PCI, the type of revascularization procedure was not significantly associated with differences in the change of rate of memory decline.
Conflict of interest statement
Figures
Comment in
-
Coronary Revascularization and Cognitive Decline: The Patient or the Procedure?JAMA. 2021 May 18;325(19):1941-1942. doi: 10.1001/jama.2021.5816. JAMA. 2021. PMID: 34003237 Free PMC article. No abstract available.
-
Association of Coronary Artery Bypass Grafting vs Percutaneous Coronary Intervention With Memory Decline in Older Adults.JAMA. 2021 Sep 28;326(12):1212-1213. doi: 10.1001/jama.2021.11976. JAMA. 2021. PMID: 34581746 No abstract available.
References
-
- Newman MF, Kirchner JL, Phillips-Bute B, et al. ; Neurological Outcome Research Group and the Cardiothoracic Anesthesiology Research Endeavors Investigators . Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med. 2001;344(6):395-402. doi: 10.1056/NEJM200102083440601 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
