

Assessment of the evolution of end-tidal carbon dioxide within chest compression pauses to detect restoration of spontaneous circulation
- PMID: 34003839
- PMCID: PMC8130954
- DOI: 10.1371/journal.pone.0251511
Assessment of the evolution of end-tidal carbon dioxide within chest compression pauses to detect restoration of spontaneous circulation
Abstract
Background: Measurement of end-tidal CO2 (ETCO2) can help to monitor circulation during cardiopulmonary resuscitation (CPR). However, early detection of restoration of spontaneous circulation (ROSC) during CPR using waveform capnography remains a challenge. The aim of the study was to investigate if the assessment of ETCO2 variation during chest compression pauses could allow for ROSC detection. We hypothesized that a decay in ETCO2 during a compression pause indicates no ROSC while a constant or increasing ETCO2 indicates ROSC.
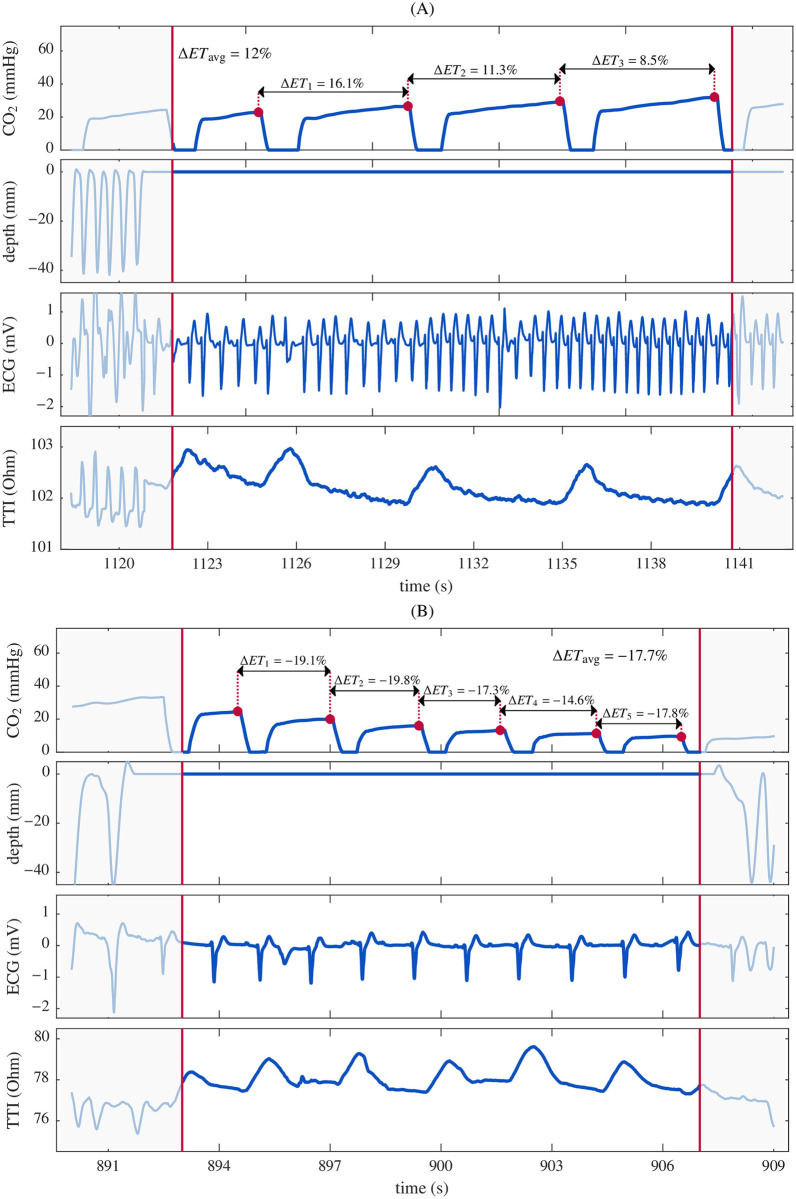
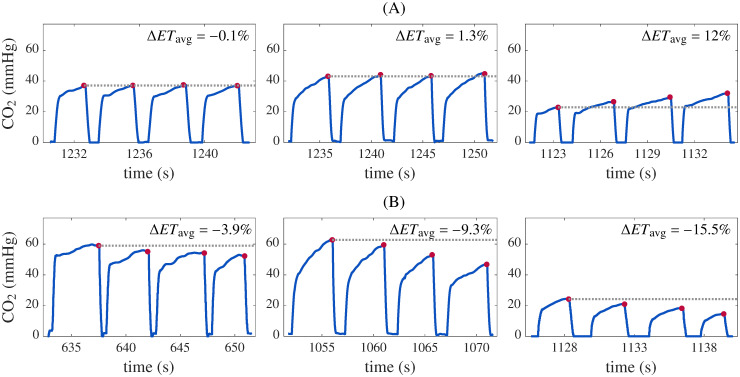
Methods: We conducted a retrospective analysis of adult out-of-hospital cardiac arrest (OHCA) episodes treated by the advanced life support (ALS). Continuous chest compressions and ventilations were provided manually. Segments of capnography signal during pauses in chest compressions were selected, including at least three ventilations and with durations less than 20 s. Segments were classified as ROSC or non-ROSC according to case chart annotation and examination of the ECG and transthoracic impedance signals. The percentage variation of ETCO2 between consecutive ventilations was computed and its average value, ΔETavg, was used as a single feature to discriminate between ROSC and non-ROSC segments.
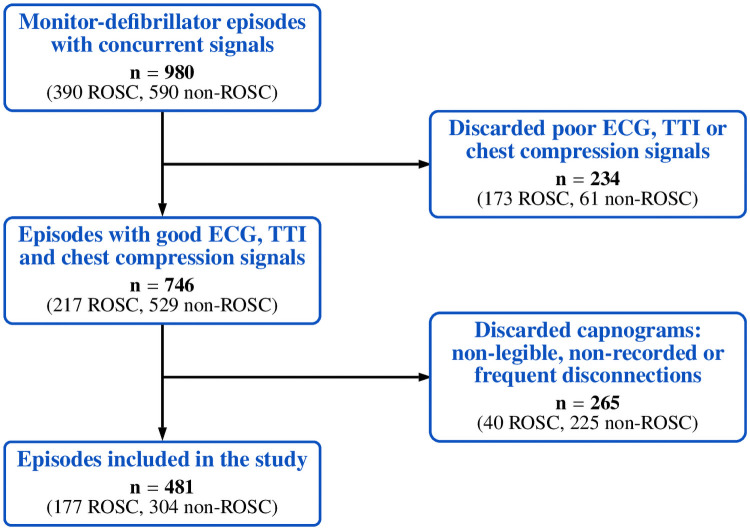
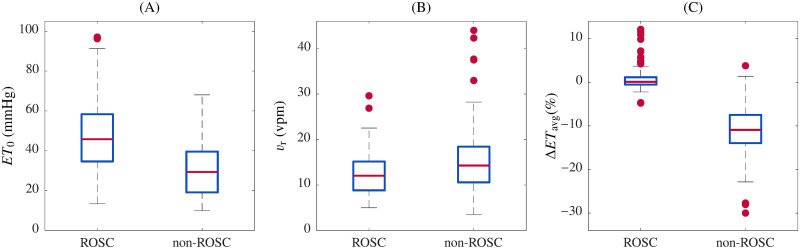
Results: A total of 384 segments (130 ROSC, 254 non-ROSC) from 205 OHCA patients (30.7% female, median age 66) were analyzed. Median (IQR) duration was 16.3 (12.9,18.1) s. ΔETavg was 0.0 (-0.7, 0.9)% for ROSC segments and -11.0 (-14.1, -8.0)% for non-ROSC segments (p < 0.0001). Best performance for ROSC detection yielded a sensitivity of 95.4% (95% CI: 90.1%, 98.1%) and a specificity of 94.9% (91.4%, 97.1%) for all ventilations in the segment. For the first 2 ventilations, duration was 7.7 (6.0, 10.2) s, and sensitivity and specificity were 90.0% (83.5%, 94.2%) and 89.4 (84.9%, 92.6%), respectively. Our method allowed for ROSC detection during the first compression pause in 95.4% of the patients.
Conclusion: Average percent variation of ETCO2 during pauses in chest compressions allowed for ROSC discrimination. This metric could help confirm ROSC during compression pauses in ALS settings.
Conflict of interest statement
Author DMGO is employed by Bexen Cardio, a Spanish medical device manufacturer. Bexen Cardio had no additional role in study funding, or study design, data collection and analysis, decision to publish, or preparation of the manuscript. This does not alter our adherence to PLOS ONE policies on sharing data and materials. The other authors declare that no competing interests exist.
Figures
Similar articles
-
Modeling the impact of ventilations on the capnogram in out-of-hospital cardiac arrest.PLoS One. 2020 Feb 5;15(2):e0228395. doi: 10.1371/journal.pone.0228395. eCollection 2020. PLoS One. 2020. PMID: 32023298 Free PMC article.
-
Contribution of chest compressions to end-tidal carbon dioxide levels generated during out-of-hospital cardiopulmonary resuscitation.Resuscitation. 2022 Oct;179:225-232. doi: 10.1016/j.resuscitation.2022.07.009. Epub 2022 Jul 11. Resuscitation. 2022. PMID: 35835250
-
Chest compressions induce errors in end-tidal carbon dioxide measurement.Resuscitation. 2020 Aug;153:195-201. doi: 10.1016/j.resuscitation.2020.05.029. Epub 2020 May 31. Resuscitation. 2020. PMID: 32492455
-
Capnography during cardiac arrest.Resuscitation. 2018 Nov;132:73-77. doi: 10.1016/j.resuscitation.2018.08.018. Epub 2018 Aug 22. Resuscitation. 2018. PMID: 30142399 Review.
-
End-Tidal Carbon Dioxide Measurement in Out-of-Hospital Cardiac Arrest as a Predictor of Return of Spontaneous Circulation: A Literature Review.Dimens Crit Care Nurs. 2024 Sep-Oct 01;43(5):253-258. doi: 10.1097/DCC.0000000000000658. Dimens Crit Care Nurs. 2024. PMID: 39074230 Review.
Cited by
-
Analysis of Emergency Medical Response Team Performance during the International Winter Championships in Emergency Medicine.Medicina (Kaunas). 2022 Nov 2;58(11):1578. doi: 10.3390/medicina58111578. Medicina (Kaunas). 2022. PMID: 36363535 Free PMC article.
-
Emergency Medicine Perspectives: The Importance of Bystanders and Their Impact on On-Site Resuscitation Measures and Immediate Outcomes of Out-of-Hospital Cardiac Arrest.J Clin Med. 2023 Oct 28;12(21):6815. doi: 10.3390/jcm12216815. J Clin Med. 2023. PMID: 37959280 Free PMC article.
-
Temporal Trends in End-Tidal Capnography and Outcomes in Out-of-Hospital Cardiac Arrest: A Secondary Analysis of a Randomized Clinical Trial.JAMA Netw Open. 2024 Jul 1;7(7):e2419274. doi: 10.1001/jamanetworkopen.2024.19274. JAMA Netw Open. 2024. PMID: 38967927 Free PMC article. Clinical Trial.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
