

Effect of CPAP Therapy on 24-Hour Intraocular Pressure-Related Pattern From Contact Lens Sensors in Obstructive Sleep Apnea Syndrome
- PMID: 34003989
- PMCID: PMC8054618
- DOI: 10.1167/tvst.10.4.10
Effect of CPAP Therapy on 24-Hour Intraocular Pressure-Related Pattern From Contact Lens Sensors in Obstructive Sleep Apnea Syndrome
Abstract
Purpose: To evaluate the effect of continuous positive airway pressure (CPAP) therapy on 24-hour intraocular pressure (IOP)-related pattern from contact lens sensors (CLS) in obstructive sleep apnea syndrome (OSAS).
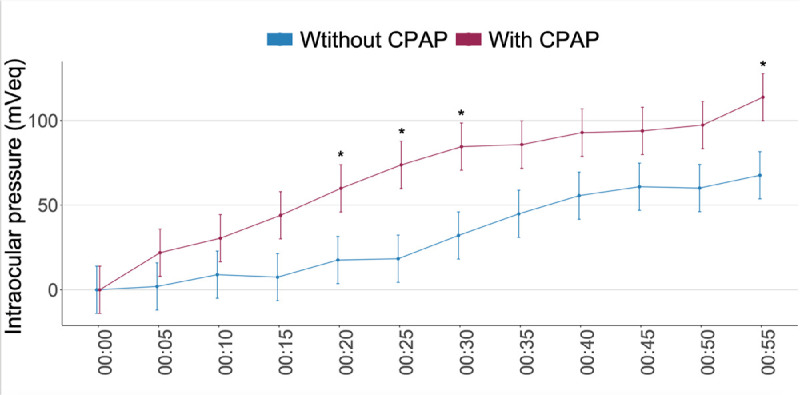
Methods: Prospective, observational, case series study. Twenty-two eyes of 22 newly diagnosed patients with severe OSAS were included. A first 24-hour CLS measurement was performed before CPAP therapy was started, and a second 24-hour CLS monitoring was performed after beginning CPAP. We analyzed the amplitude and the maximum and minimum IOP-related values (m Veq). We also analyzed IOP-related measurements at five-minute intervals throughout the first hour of nocturnal acrophase, starting from when the patient fell asleep.
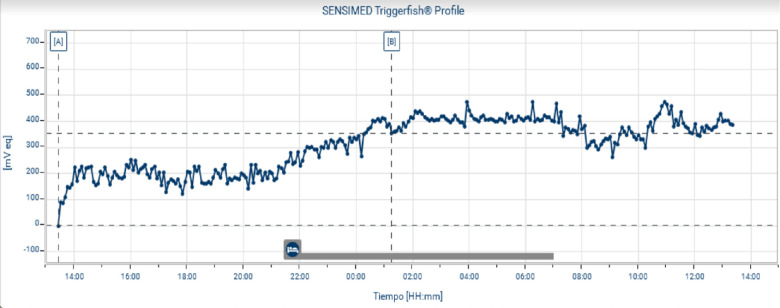
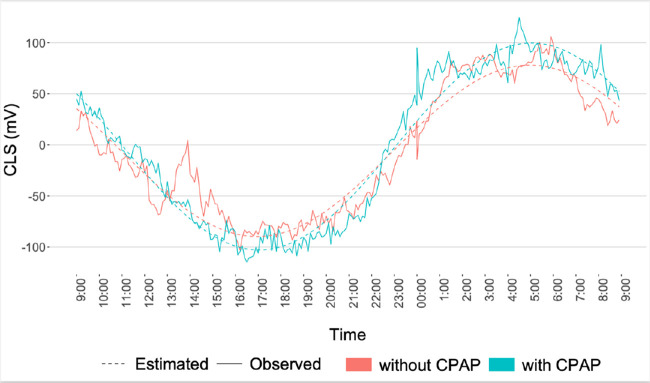
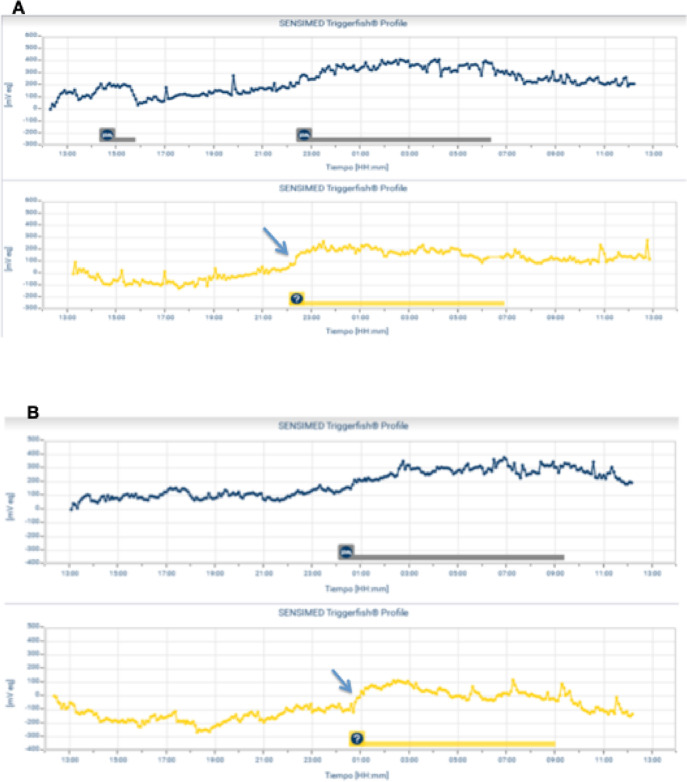
Results: The baseline measurements showed significant fluctuations in the IOP, with the highest IOP readings being recorded at night (nocturnal acrophase) in 17 of 22 patients (77.27%). Nocturnal acrophase began when the patients laid down to sleep. During CPAP therapy, the patients showed a more marked increase in IOP in the initial phase of nocturnal acrophase, with significant differences at 20, 25, 30, and 55 minutes (P < 0.05).
Conclusions: Most of patients with severe OSAS exhibited a nocturnal acrophase and the highest IOP readings at night. CPAP was associated with additional increase in IOP-related pattern for at least the first hour of CPAP use.
Translational relevance: Our results suggest that CPAP was associated with additional increase in IOP during the initial phase of nocturnal acrophase. This effect could be important in the management of patients with OSAS and glaucomatous progression.
Conflict of interest statement
Disclosure:
Figures

References
-
- Sanchez-de-la-Torre M, Campos-Rodriguez F, Barbé F. Obstructive sleep apnoea and cardiovascular disease. Lancet Respir Med. 2013; 1: 61–72. - PubMed
-
- Atwood CW, Strollo PJ, Givelber R. In: Medical Therapy for Obstructive Sleep Apnea, in Principles and Practice of Sleep Medicine. Kryger MH, Roth T, Dement WC, eds. Vol. 5. Saunders; Chicago: 2005.
-
- Muniesa MJ, Huerva V, Sánchez-de-la-Torre M, et al. .. The relationship between floppy eyelid syndrome and obstructive sleep apnoea. Br J Ophthalmol. 2013; 97: 1387–1390. - PubMed
-
- Culbertson WW, Tseng SCG. Corneal disorders in floppy eyelid syndrome. Cornea. 1994; 13: 33–42. - PubMed
-
- Mojon DS, Mathis J, Zulauf M, et al. .. Optic neuropathy associated with sleep apnea syndrome. Ophthalmology. 1998; 105: 874–877. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
