

How does the effectiveness of strategies to improve healthcare provider practices in low-income and middle-income countries change after implementation? Secondary analysis of a systematic review
- PMID: 34006598
- PMCID: PMC8784997
- DOI: 10.1136/bmjqs-2020-011717
How does the effectiveness of strategies to improve healthcare provider practices in low-income and middle-income countries change after implementation? Secondary analysis of a systematic review
Abstract
Background: A recent systematic review evaluated the effectiveness of strategies to improve healthcare provider (HCP) performance in low-income and middle-income countries. The review identified strategies with varying effects, including in-service training, supervision and group problem-solving. However, whether their effectiveness changed over time remained unclear. In particular, understanding whether effects decay over time is crucial to improve sustainability.
Methods: We conducted a secondary analysis of data from the aforementioned review to explore associations between time and effectiveness. We calculated effect sizes (defined as percentage-point (%-point) changes) for HCP practice outcomes (eg, percentage of patients correctly treated) at each follow-up time point after the strategy was implemented. We estimated the association between time and effectiveness using random-intercept linear regression models with time-specific effect sizes clustered within studies and adjusted for baseline performance.
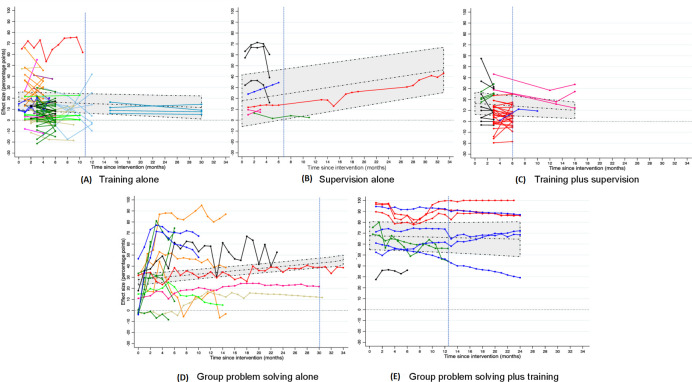
Results: The primary analysis included 37 studies, and a sensitivity analysis included 77 additional studies. For training, every additional month of follow-up was associated with a 0.19 %-point decrease in effectiveness (95% CI: -0.36 to -0.03). For training combined with supervision, every additional month was associated with a 0.40 %-point decrease in effectiveness (95% CI: -0.68 to -0.12). Time trend results for supervision were inconclusive. For group problem-solving alone, time was positively associated with effectiveness, with a 0.50 %-point increase in effect per month (95% CI: 0.37 to 0.64). Group problem-solving combined with training was associated with large improvements, and its effect was not associated with time.
Conclusions: Time trends in the effectiveness of different strategies to improve HCP practices vary among strategies. Programmes relying solely on in-service training might need periodical refresher training or, better still, consider combining training with group problem-solving. Although more high-quality research is needed, these results, which are important for decision-makers as they choose which strategies to use, underscore the utility of studies with multiple post-implementation measurements so sustainability of the impact on HCP practices can be assessed.
Keywords: health services research; implementation science; performance measures; quality improvement; standards of care.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
The effectiveness of supervision strategies to improve health care provider practices in low- and middle-income countries: secondary analysis of a systematic review.Hum Resour Health. 2022 Jan 6;20(1):1. doi: 10.1186/s12960-021-00683-z. Hum Resour Health. 2022. PMID: 34991608 Free PMC article.
-
The effectiveness of training strategies to improve healthcare provider practices in low-income and middle-income countries.BMJ Glob Health. 2021 Jan;6(1):e003229. doi: 10.1136/bmjgh-2020-003229. BMJ Glob Health. 2021. PMID: 33452138 Free PMC article.
-
Effectiveness of strategies to improve health-care provider practices in low-income and middle-income countries: a systematic review.Lancet Glob Health. 2018 Nov;6(11):e1163-e1175. doi: 10.1016/S2214-109X(18)30398-X. Epub 2018 Oct 8. Lancet Glob Health. 2018. PMID: 30309799 Free PMC article.
-
A systematic review of the effectiveness of strategies to improve health care provider performance in low- and middle-income countries: Methods and descriptive results.PLoS One. 2019 May 31;14(5):e0217617. doi: 10.1371/journal.pone.0217617. eCollection 2019. PLoS One. 2019. PMID: 31150458 Free PMC article.
-
The effectiveness of the quality improvement collaborative strategy in low- and middle-income countries: A systematic review and meta-analysis.PLoS One. 2019 Oct 3;14(10):e0221919. doi: 10.1371/journal.pone.0221919. eCollection 2019. PLoS One. 2019. PMID: 31581197 Free PMC article.
Cited by
-
Insights from national stakeholders and health workers on learning and performance interventions in immunisation programs: a multi-country situational analysis.J Glob Health. 2025 Mar 28;15:04109. doi: 10.7189/jogh.15.04109. J Glob Health. 2025. PMID: 40153334 Free PMC article.
-
Evaluation of a massive open online course for just-in-time training of healthcare workers.Front Public Health. 2024 Oct 1;12:1395931. doi: 10.3389/fpubh.2024.1395931. eCollection 2024. Front Public Health. 2024. PMID: 39411488 Free PMC article.
-
The effectiveness of supervision strategies to improve health care provider practices in low- and middle-income countries: secondary analysis of a systematic review.Hum Resour Health. 2022 Jan 6;20(1):1. doi: 10.1186/s12960-021-00683-z. Hum Resour Health. 2022. PMID: 34991608 Free PMC article.
-
Cost-effectiveness and sustainability of improved hospital oxygen systems in Nigeria.BMJ Glob Health. 2022 Aug;7(8):e009278. doi: 10.1136/bmjgh-2022-009278. BMJ Glob Health. 2022. PMID: 35948344 Free PMC article.
-
Lessons Learnt Delivering a Novel Infectious Diseases National Training Programme to Timor‑Leste's Primary Care Workforce.Ann Glob Health. 2024 Nov 6;90(1):66. doi: 10.5334/aogh.4352. eCollection 2024. Ann Glob Health. 2024. PMID: 39525392 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous