

Comprehensive Review of AL amyloidosis: some practical recommendations
- PMID: 34006856
- PMCID: PMC8130794
- DOI: 10.1038/s41408-021-00486-4
Comprehensive Review of AL amyloidosis: some practical recommendations
Abstract
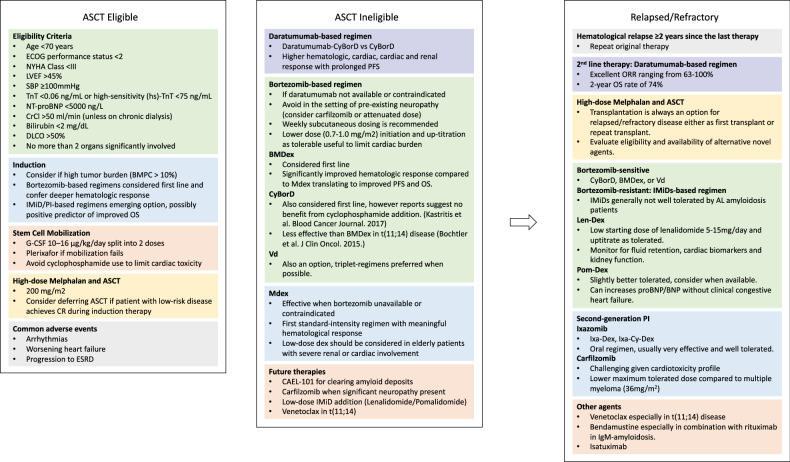
Amyloid light chain (AL) amyloidosis is among the more common and more severe of the amyloidoses usually involving the slow proliferation of a bone-marrow-residing plasma cell (PC) clone and the secretion of unstable immunoglobulin-free light chains (FLC) that infiltrate peripheral tissues and result in detrimental end-organ damage. Disease presentation is rather vague, and the hallmark of treatment is early diagnosis before irreversible end-organ damage. Once diagnosed, treatment decision is transplant-driven whereby ~20% of patients are eligible for autologous stem cell transplantation (ASCT) with or without bortezomib-based induction. In the setting of ASCT-ineligibility, bortezomib plays a central role in upfront treatment with the recent addition of daratumumab to the current emerging standard of care. In general, management of AL amyloidosis is aimed at achieving deep, durable responses with very close monitoring for early detection of relapse/refractory disease. This article provides a comprehensive review of the management of patients with AL amyloidosis including goals of therapy, current treatment guidelines in the setting of both ASCT-eligibility and ineligibility, treatment response monitoring recommendations, toxicity management, and treatment of relapse/refractory disease.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
