

Intratumoural administration and tumour tissue targeting of cancer immunotherapies
- PMID: 34006998
- PMCID: PMC8130796
- DOI: 10.1038/s41571-021-00507-y
Intratumoural administration and tumour tissue targeting of cancer immunotherapies
Abstract
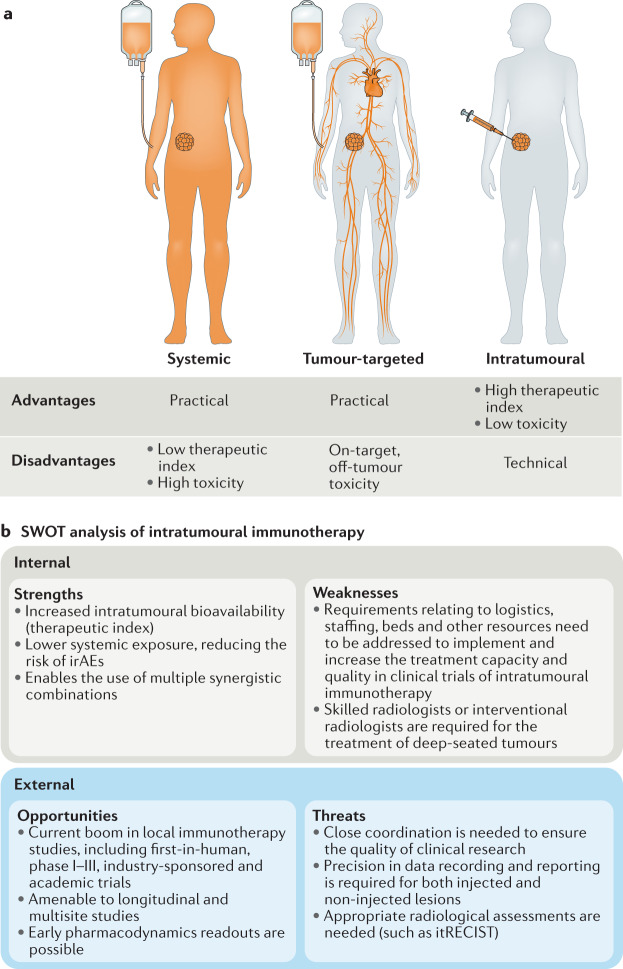
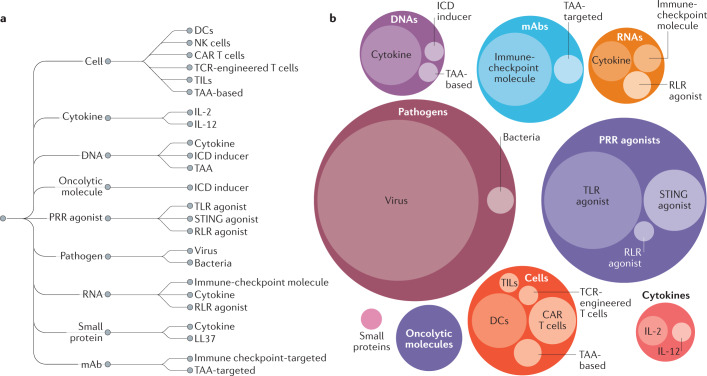
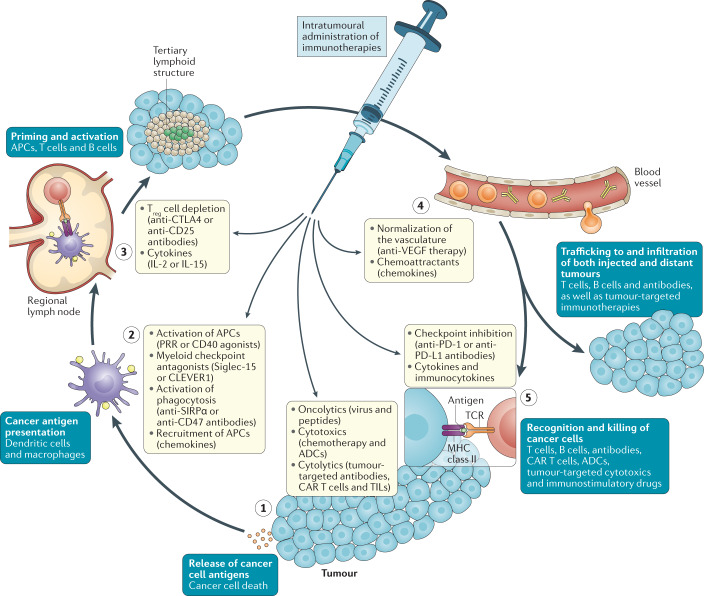
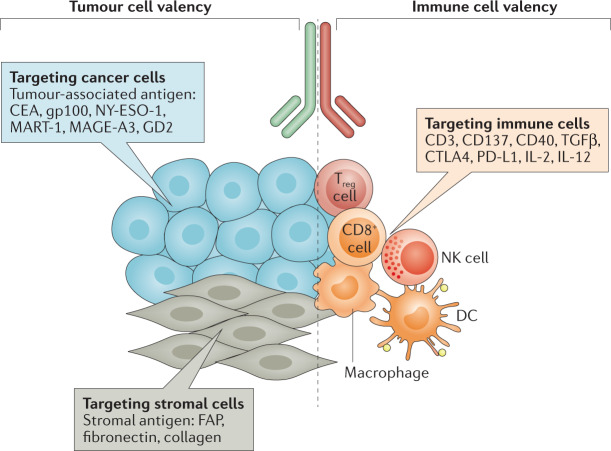
Immune-checkpoint inhibitors and chimeric antigen receptor (CAR) T cells are revolutionizing oncology and haematology practice. With these and other immunotherapies, however, systemic biodistribution raises safety issues, potentially requiring the use of suboptimal doses or even precluding their clinical development. Delivering or attracting immune cells or immunomodulatory factors directly to the tumour and/or draining lymph nodes might overcome these problems. Hence, intratumoural delivery and tumour tissue-targeted compounds are attractive options to increase the in situ bioavailability and, thus, the efficacy of immunotherapies. In mouse models, intratumoural administration of immunostimulatory monoclonal antibodies, pattern recognition receptor agonists, genetically engineered viruses, bacteria, cytokines or immune cells can exert powerful effects not only against the injected tumours but also often against uninjected lesions (abscopal or anenestic effects). Alternatively, or additionally, biotechnology strategies are being used to achieve higher functional concentrations of immune mediators in tumour tissues, either by targeting locally overexpressed moieties or engineering 'unmaskable' agents to be activated by elements enriched within tumour tissues. Clinical trials evaluating these strategies are ongoing, but their development faces issues relating to the administration methodology, pharmacokinetic parameters, pharmacodynamic end points, and immunobiological and clinical response assessments. Herein, we discuss these approaches in the context of their historical development and describe the current landscape of intratumoural or tumour tissue-targeted immunotherapies.
© 2021. Springer Nature Limited.
Conflict of interest statement
I.M. has received research grants from Alligator, Bioncotech, Bristol Myers Squibb (BMS), Leadartis, Pfizer and Roche; has received speaker’s bureau honoraria from MSD; and is a consultant or advisory board member for Alligator, AstraZeneca, Bayer, Bioncotech, BMS, F-Star, Genmab, Gossamer, Merck Serono, Numab, Pieris and Roche. E.C. is a consultant or advisory board member for AstraZeneca, Beigene, BMS, MSD and Roche. S.C. has received honoraria from Amgen, AstraZeneca, BMS, Janssen, Merck, MSD, Novartis and Roche; is an advisory board member for Amgen and AstraZeneca; has received funding for travel and conference attendance from AstraZeneca, MSD and Roche; and has received research grants from AstraZeneca, BMS, Boehringer Ingelheim, Janssen-Cilag, Merck, Novartis, Onxeo, Pfizer, Roche and Sanofi, and non-financial research support (investigational drugs) from AstraZeneca, Bayer, BMS, Boehringer Ingelheim, Medimmune, Merck, NH TherAGuiX, Onxeo, Pfizer and Roche. S.C. has been a principal investigator of academic or industry-sponsored clinical trials of intratumoural immunotherapies for Abbvie, AstraZeneca/Medimmune, BMS, Eisai/H3 Biomedicine, IDERA, Lytix Biopharma, MSD, Nanobiotix and Sanofi/BioNTech. A.M. has been a principal investigator of academic or industry-sponsored clinical trials of intratumoural immunotherapies from AstraZeneca, BMS, Eisai, IDERA, Lytix Biopharma, Merck/MSD, Roche and Transgene; is a member of the Data Safety and Monitoring Board of a trial of a intratumoural TLR3 agonist sponsored by Oncovir (NCT02423863); and has participated in scientific advisory boards or has provided consultancy services on the topic of intratumoural immunotherapies for Amgen, AstraZeneca, Banque Pour l’Investissement, Bayer, Eisai, eTheRNA, Lytix Biopharma, Medincell, MSD, Novartis, Oncosec, Pillar Partners, Rigontec and Sanofi/BioNTech. M.A. declares no competing interests.
Figures
References
-
- Melero I, Rouzaut A, Motz GT, Coukos G. T-cell and NK-cell infiltration into solid tumors: a key limiting factor for efficacious cancer immunotherapy. Cancer Discov. 2014;4:522–526. doi: 10.1158/2159-8290.CD-13-0985. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
