

Qindan Capsule Attenuates Myocardial Hypertrophy and Fibrosis in Pressure Overload-Induced Mice Involving mTOR and TGF- β 1/Smad Signaling Pathway Inhibition
- PMID: 34007292
- PMCID: PMC8102107
- DOI: 10.1155/2021/5577875
Qindan Capsule Attenuates Myocardial Hypertrophy and Fibrosis in Pressure Overload-Induced Mice Involving mTOR and TGF- β 1/Smad Signaling Pathway Inhibition
Abstract
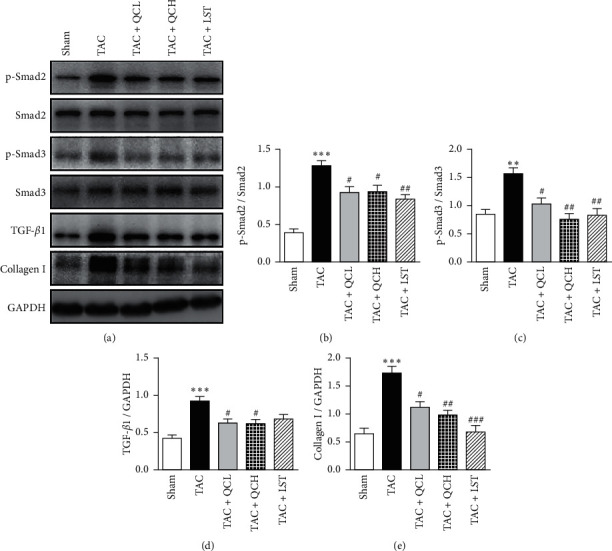
Qindan capsule (QC), a traditional Chinese medicine compound, has been used to treat hypertension in the clinic for over 30 years. It is still not known about the effects of QC on pressure overload-induced cardiac remodeling. Hence, this study aims to investigate the effects of QC on pressure overload-induced cardiac hypertrophy, fibrosis, and heart failure in mice and to determine the possible mechanisms. Transverse aortic constriction (TAC) surgery was used to induce cardiac hypertrophy and heart failure in C57BL/6 mice. Mice were treated with QC or losartan for 8 weeks after TAC surgery. Cardiac function indexes were evaluated with transthoracic echocardiography. Cardiac pathology was detected using HE and Masson's trichrome staining. Cardiomyocyte ultrastructure was detected using transmission electron microscopy. Hypertrophy-related fetal gene expression was investigated using real-time RT-PCR. The expression of 8-OHdG and the concentration of MDA and Ang-II were assessed by immunohistochemistry stain and ELISA assay, respectively. The total and phosphorylated protein levels of mTOR, p70S6K, 4EBP1, Smad2, and Smad3 and the expression of TGF-β1 and collagen I were measured using western blot. The results showed that low- and high-dose QC improved pressure overload-induced cardiac hypertrophy, fibrosis, and dysfunction. QC inhibited ANP, BNP, and β-MHC mRNA expression in failing hearts. QC improved myocardial ultrastructure after TAC surgery. Furthermore, QC downregulated the expression of 8-OHdG and the concentration of MDA, 15-F2t-IsoP, and Ang-II in heart tissues after TAC surgery. We also found that QC inhibited the phosphorylation of mTOR, p70S6K, and 4EBP1 and the expression of TGF-β1, p-Smad2, p-Smad3, and collagen I in pressure overload-induced failing hearts. These data indicate that QC has direct benefic effects on pressure overload-induced cardiac hypertrophy, fibrosis, and dysfunction. The protective effects of QC involve prevention of increased oxidative stress injury and Ang-II levels and inhibition of mTOR and TGF-β1/Smad pathways in failing hearts.
Copyright © 2021 Wenwu Bai et al.
Conflict of interest statement
The authors declare that there are no conflicts of interest associated with the manuscript.
Figures





References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
