

Energy expenditure and physical activity in COPD by doubly labelled water method and an accelerometer
- PMID: 34007842
- PMCID: PMC8093485
- DOI: 10.1183/23120541.00407-2020
Energy expenditure and physical activity in COPD by doubly labelled water method and an accelerometer
Abstract
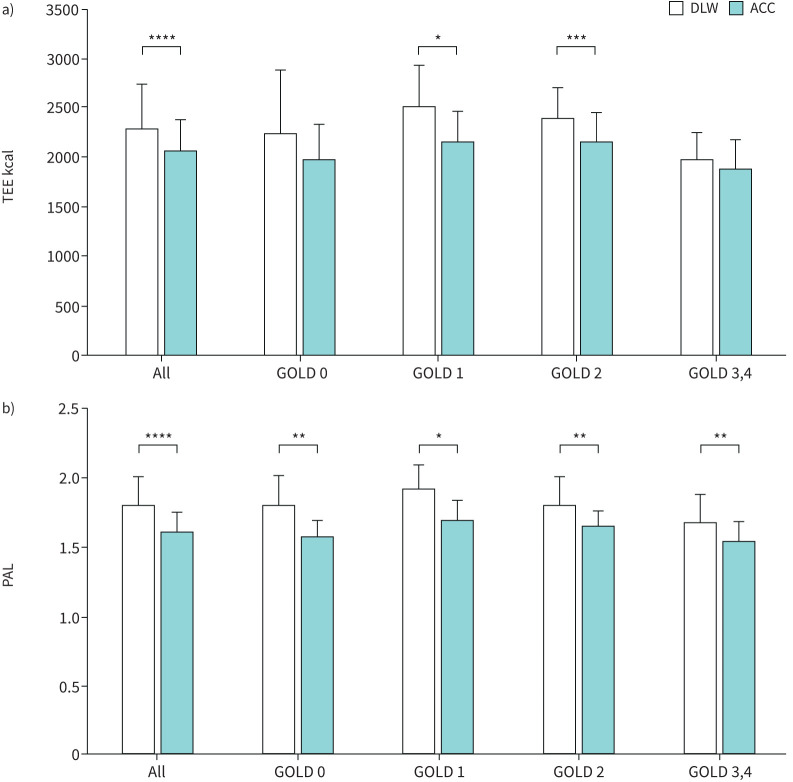
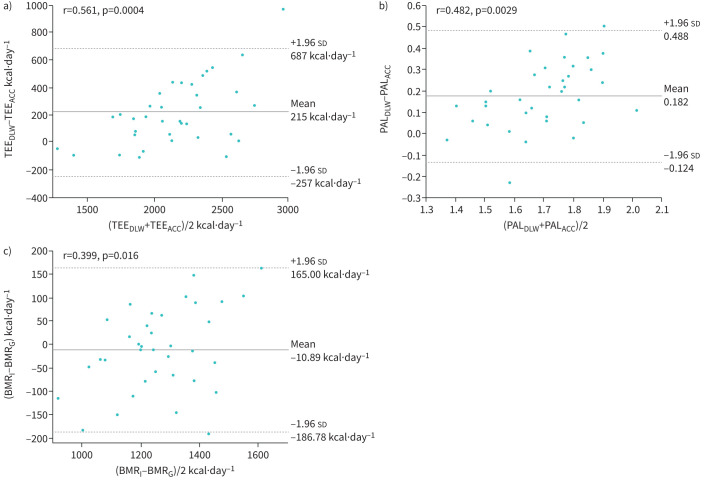
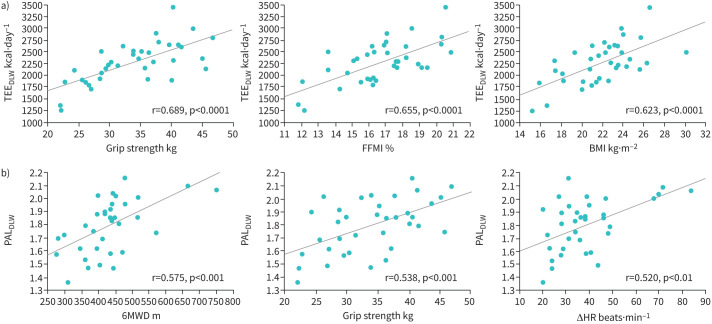
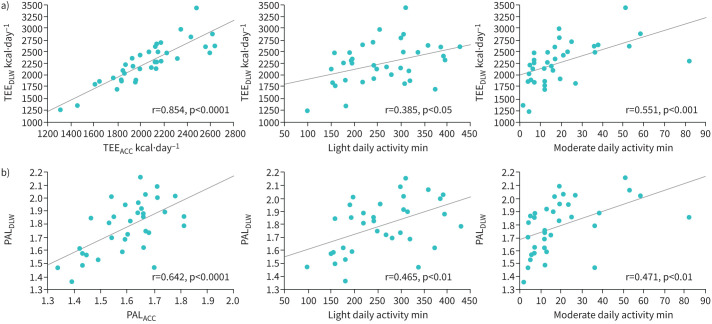
Although weight loss suggests poor prognosis of COPD, only a few studies have examined total energy expenditure (TEE) or physical activity level (PAL) using the doubly labelled water (DLW) method. We evaluated TEE and PAL using the DLW method together with a triaxial accelerometer to elucidate the relationships between TEE, PAL and clinical parameters leading to a practical means of monitoring COPD physical status. This study evaluated 50- to 79-year-old male patients with mild to very severe COPD (n=28) or at risk for COPD (n=8). TEE, activity energy expenditure for 2 weeks and basal metabolic rate were measured by DLW, an accelerometer and indirect calorimetry, respectively. All patients underwent pulmonary function, chest-computed tomography, 6-min walk test, body composition and grip strength tests. Relationships between indices of energy expenditure and clinical parameters were analysed. Bland-Altman analysis was used to examine the agreement of TEE and PAL between the DLW method and the accelerometer. TEE and PAL using DLW in the total population were 2273±445 kcal·day-1 and 1.80±0.20, respectively. TEE by DLW correlated well with that from the accelerometer and grip strength (p<0.0001), and PAL by DLW correlated well with that from the accelerometer (p<0.0001), grip strength and 6-min walk distance (p<0.001) among various clinical parameters. However, the accelerometer underestimated TEE (215±241 kcal·day-1) and PAL (0.18±0.16), with proportional biases in both indices. TEE and PAL can be estimated by accelerometer in patients with COPD if systematic errors and relevant clinical factors such as muscle strength and exercise capacity are accounted for.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: H. Sato has nothing to disclose. Conflict of interest: H. Nakamura reports grants from the Japan Agency for Medical Research and Development (AMED) during the conduct of the study. Conflict of interest: Y. Nishida has nothing to disclose. Conflict of interest: T. Shirahata has nothing to disclose. Conflict of interest: S. Yogi has nothing to disclose. Conflict of interest: T. Akagami has nothing to disclose. Conflict of interest: M. Soma has nothing to disclose. Conflict of interest: K. Inoue has nothing to disclose. Conflict of interest: M. Niitsu has nothing to disclose. Conflict of interest: T. Mio has nothing to disclose. Conflict of interest: T. Miyashita has nothing to disclose. Conflict of interest: M. Nagata has nothing to disclose. Conflict of interest: S. Nakae has nothing to disclose. Conflict of interest: Y. Yamada has nothing to disclose. Conflict of interest: S. Tanaka reports grants from the Japan Agency for Medical Research and Development (AMED) during the conduct of the study. Conflict of interest: F. Katsukawa reports grants from the Japan Agency for Medical Research and Development (AMED) during the conduct of the study.
Figures
Similar articles
-
Validity of the Use of a Triaxial Accelerometer and a Physical Activity Questionnaire for Estimating Total Energy Expenditure and Physical Activity Level among Elderly Patients with Type 2 Diabetes Mellitus: CLEVER-DM Study.Ann Nutr Metab. 2020;76(1):62-72. doi: 10.1159/000506223. Epub 2020 Mar 13. Ann Nutr Metab. 2020. PMID: 32172232
-
The product of trunk muscle area and density on the CT image is a good indicator of energy expenditure in patients with or at risk for COPD.Respir Res. 2021 Jan 15;22(1):18. doi: 10.1186/s12931-021-01621-2. Respir Res. 2021. PMID: 33451329 Free PMC article.
-
Validity of a triaxial accelerometer and simplified physical activity record in older adults aged 64-96 years: a doubly labeled water study.Eur J Appl Physiol. 2018 Oct;118(10):2133-2146. doi: 10.1007/s00421-018-3944-6. Epub 2018 Jul 17. Eur J Appl Physiol. 2018. PMID: 30019086
-
Comparison of total and activity energy expenditure estimates from physical activity questionnaires and doubly labelled water: a systematic review and meta-analysis.Br J Nutr. 2021 May 14;125(9):983-997. doi: 10.1017/S0007114520003049. Epub 2020 Jul 28. Br J Nutr. 2021. PMID: 32718378
-
Doubly labelled water for determining total energy expenditure in adult critically ill and acute care hospitalized inpatients: A scoping review.Clin Nutr. 2022 Feb;41(2):424-432. doi: 10.1016/j.clnu.2021.12.017. Epub 2021 Dec 16. Clin Nutr. 2022. PMID: 35007811
Cited by
-
Prediction of the Physical Activity Level of Community-Dwelling Older Japanese Adults with a Triaxial Accelerometer Containing a Classification Algorithm for Ambulatory and Non-Ambulatory Activities.Sensors (Basel). 2023 May 22;23(10):4960. doi: 10.3390/s23104960. Sensors (Basel). 2023. PMID: 37430874 Free PMC article.
-
Individually optimized estimation of energy expenditure in rescue workers using a tri-axial accelerometer and heart rate monitor.Front Physiol. 2024 Feb 15;15:1322881. doi: 10.3389/fphys.2024.1322881. eCollection 2024. Front Physiol. 2024. PMID: 38434137 Free PMC article.
-
Effects of exercise intensity on nutritional status, body composition, and energy balance in patients with COPD: a randomized controlled trial.BMC Pulm Med. 2025 Jan 24;25(1):34. doi: 10.1186/s12890-024-03448-1. BMC Pulm Med. 2025. PMID: 39856592 Free PMC article. Clinical Trial.
-
Energy expenditure estimation during activities of daily living in middle-aged and older adults using an accelerometer integrated into a hearing aid.Front Digit Health. 2024 Jun 17;6:1400535. doi: 10.3389/fdgth.2024.1400535. eCollection 2024. Front Digit Health. 2024. PMID: 38952746 Free PMC article.
-
Impact of non-exercise activity thermogenesis on physical activity in patients with COPD.Sci Prog. 2022 Jul-Sep;105(3):368504221117064. doi: 10.1177/00368504221117064. Sci Prog. 2022. PMID: 36082951 Free PMC article.
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease 2020 Report. https://goldcopd.org/wp-content/uploads/2019/11/GOLD-2020-REPORT-ver1.0w... - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources