

Impact of PTV margin reduction (2 mm to 0 mm) on pseudoprogression in stereotactic radiotherapy of solitary brain metastases
- PMID: 34007906
- PMCID: PMC8111033
- DOI: 10.1016/j.tipsro.2021.02.008
Impact of PTV margin reduction (2 mm to 0 mm) on pseudoprogression in stereotactic radiotherapy of solitary brain metastases
Abstract
Purpose: To determine the influence of PTV-margin (0 mm versus 2 mm) on the incidence of pseudoprogression (PP) and local tumour control (LC) in patients treated with stereotactic radiotherapy (SRT) for solitary brain metastases.
Methods: Patients were treated on Novalis LINAC. Three dose schedules were used depending on the PTV-size. The PTV-margin was 2-mm prior to 2015 and 0-mm thereafter. MRI-scans were made every three months including a perfusion MRI-scan when pseudoprogression was suspected. We examined the relation of pseudoprogression and local control with the size of PTV-margin. Besides this, the association of dose-volume data of the whole brain (minus GTV) and pseudoprogression was investigated.
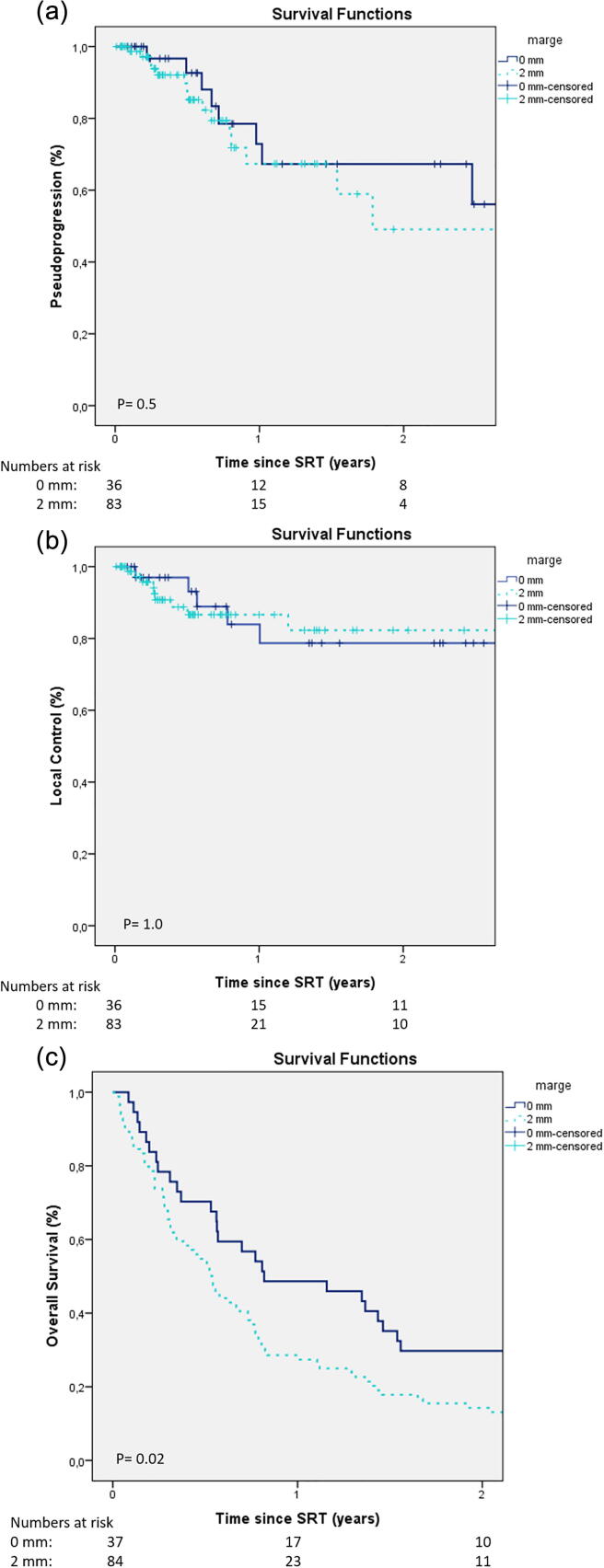
Results: 121 patients were analyzed (2-mm margin in 84 patients; 0-mm margin in 37 patients). There was no difference in GTV (7.6 cc versus 9.1 cc p = 0.2). At 24 months there was no difference in incidence of pseudoprogression (49% and versus 33%, p = 0.5) and local control in the 2-mm and 0-mm group (82% and versus 79%, p = 1.0). The size of PTV-margin was not associated with PP. Both margin and volume of brain receiving 12 Gy (V12) were not associated with pseudoprogression in patients treated with single fraction.
Conclusions: PTV-margin reduction did not reduce the incidence of pseudoprogression in LINAC-based-SRT for single brain metastases. We did not find a significant association of GTV-PTV margin or V12Gy with the incidence of pseudoprogression in solitary metastases treated with a single fraction. LC rates were similar, indicating margin reduction seems to be safe.
Keywords: Brain metastases; Margins; Pseudoprogression; Stereotactic radiotherapy.
© 2021 The Authors. Published by Elsevier B.V. on behalf of European Society for Radiotherapy & Oncology.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


Similar articles
-
Interfractional target changes in brain metastases during 13-fraction stereotactic radiotherapy.Radiat Oncol. 2021 Jul 28;16(1):140. doi: 10.1186/s13014-021-01869-4. Radiat Oncol. 2021. PMID: 34321033 Free PMC article.
-
The impact of histology and delivered dose on local control of spinal metastases treated with stereotactic radiosurgery.Neurosurg Focus. 2017 Jan;42(1):E6. doi: 10.3171/2016.9.FOCUS16369. Neurosurg Focus. 2017. PMID: 28041329 Free PMC article.
-
Linac-based VMAT radiosurgery for multiple brain lesions: comparison between a conventional multi-isocenter approach and a new dedicated mono-isocenter technique.Radiat Oncol. 2018 Mar 5;13(1):38. doi: 10.1186/s13014-018-0985-2. Radiat Oncol. 2018. PMID: 29506539 Free PMC article.
-
[Hypofractionated stereotactic radiotherapy for brain metastases].Cancer Radiother. 2010 Apr;14(2):119-27. doi: 10.1016/j.canrad.2009.10.004. Epub 2009 Dec 8. Cancer Radiother. 2010. PMID: 20004125 Review. French.
-
IMRT for prostate cancer: defining target volume based on correlated pathologic volume of disease.Int J Radiat Oncol Biol Phys. 2003 May 1;56(1):184-91. doi: 10.1016/s0360-3016(03)00085-3. Int J Radiat Oncol Biol Phys. 2003. PMID: 12694837 Review.
Cited by
-
Dosimetric Analysis of Intra-Fraction Motion Detected by Surface-Guided Radiation Therapy During Linac Stereotactic Radiosurgery.Adv Radiat Oncol. 2022 Dec 27;8(3):101151. doi: 10.1016/j.adro.2022.101151. eCollection 2023 May-Jun. Adv Radiat Oncol. 2022. PMID: 36691448 Free PMC article.
-
Spatial accuracy of dose delivery significantly impacts the planning target volume margin in linear accelerator-based intracranial stereotactic radiosurgery.Sci Rep. 2025 Jan 29;15(1):3608. doi: 10.1038/s41598-025-87769-z. Sci Rep. 2025. PMID: 39875508 Free PMC article.
-
Local recurrence and radionecrosis after single-isocenter multiple targets stereotactic radiotherapy for brain metastases.Sci Rep. 2025 May 5;15(1):15722. doi: 10.1038/s41598-025-01034-x. Sci Rep. 2025. PMID: 40325083 Free PMC article.
-
Initial Experience of Implementing a Pre-treatment Dry Run for HyperArc Stereotactic Radiosurgery Treatments With Optical Surface Imaging for Intra-fraction Motion Monitoring.Cureus. 2024 Nov 6;16(11):e73124. doi: 10.7759/cureus.73124. eCollection 2024 Nov. Cureus. 2024. PMID: 39650945 Free PMC article.
-
Treatment planning with high-resolution 3D dose maps in preclinical and translational synchrotron microbeam radiation therapy.Phys Imaging Radiat Oncol. 2024 Feb 28;30:100565. doi: 10.1016/j.phro.2024.100565. eCollection 2024 Apr. Phys Imaging Radiat Oncol. 2024. PMID: 39474259 Free PMC article.
References
-
- Habets EJJ, Dirven L, Wiggenraad RG, Verbeek-De Kanter A, Lycklama À Nijeholt GJ, Zwinkels H, et al. Neurocognitive functioning and health-related quality of life in patients treated with stereotactic radiotherapy for brain metastases: A prospective study. Neuro Oncol 2016; 18. doi: 10.1093/neuonc/nov186. - PMC - PubMed
-
- Patchell RA. The management of brain metastases. Cancer Treat Rev 2003; 29: 533–40. doi: 10.1016/S0305-7372(03)00105-1. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
