

Normal Adrenal and Thyroid Function in Patients Who Survive COVID-19 Infection
- PMID: 34008009
- PMCID: PMC8194556
- DOI: 10.1210/clinem/dgab349
Normal Adrenal and Thyroid Function in Patients Who Survive COVID-19 Infection
Abstract
Context: The COVID-19 pandemic continues to exert an immense burden on global health services. Moreover, up to 63% of patients experience persistent symptoms, including fatigue, after acute illness. Endocrine systems are vulnerable to the effects of COVID-19 as many glands express the ACE2 receptor, used by the SARS-CoV-2 virion for cellular access. However, the effects of COVID-19 on adrenal and thyroid gland function after acute COVID-19 remain unknown.
Objective: Our objectives were to evaluate adrenal and thyroid gland function in COVID-19 survivors.
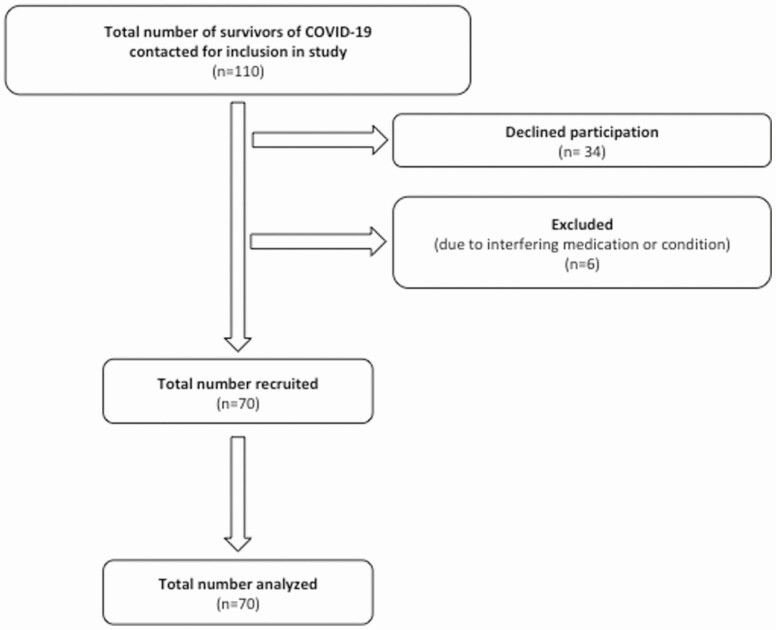
Methods: A prospective, observational study was undertaken at the Clinical Research Facility, Imperial College NHS Healthcare Trust, including 70 patients ≥18 years of age, at least 3 months after diagnosis of COVID-19. Participants attended a research study visit (8:00-9:30 am), during which a short Synacthen test (250 µg IV bolus) and thyroid function assessments were performed.
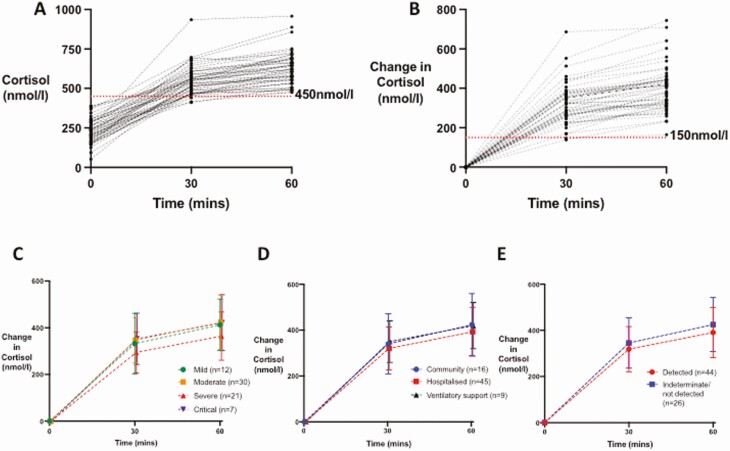
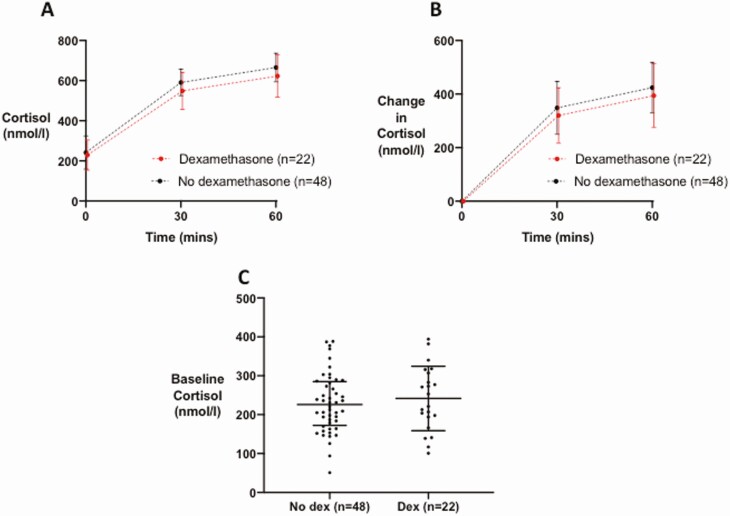
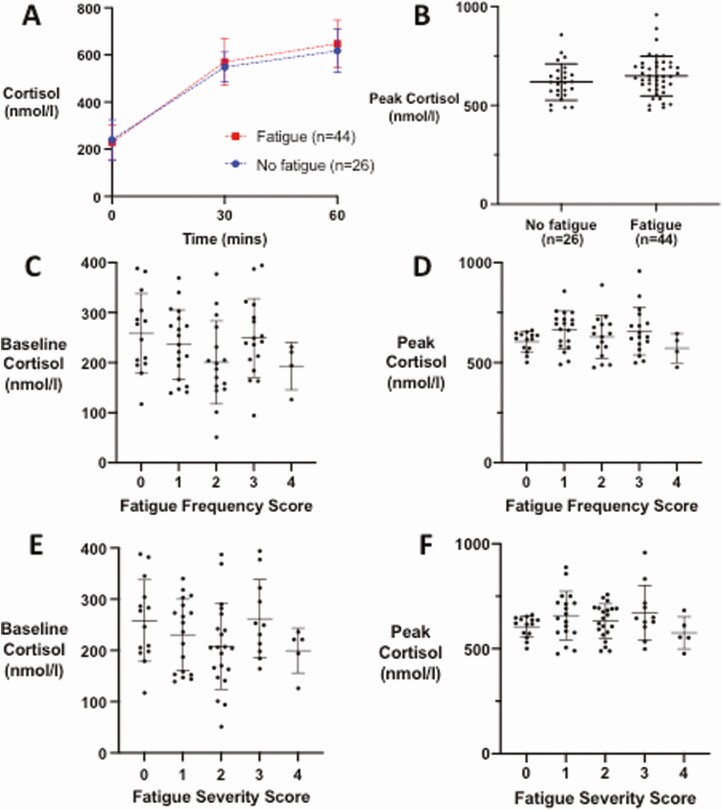
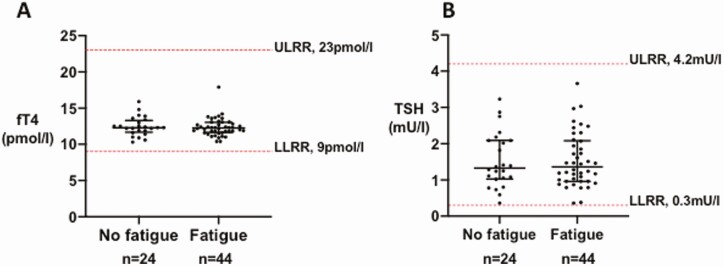
Results: All patients had a peak cortisol ≥450 nmol/L after Synacthen, consistent with adequate adrenal reserve. Basal and peak serum cortisol did not differ according to disease severity or history of dexamethasone treatment during COVID-19. There was no difference in baseline or peak cortisol after Synacthen or in thyroid function tests, or thyroid status, in patients with fatigue (n = 44) compared to those without (n = 26).
Conclusion: Adrenal and thyroid function ≥3 months after presentation with COVID-19 was preserved. While a significant proportion of patients experienced persistent fatigue, their symptoms were not accounted for by alterations in adrenal or thyroid function. These findings have important implications for the clinical care of patients after COVID-19.
Keywords: COVID-19; SARS-CoV-2; adrenal function; adrenal insufficiency; thyroid function; thyroid gland.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- World Health Organization. World Health Organisation Coronavirus Disease (COVID-19) Dashboard. Accessed February 11, 2021. https://covid19.who.int
-
- Donoghue M, Hsieh F, Baronas E, et al. . A novel angiotensin-converting enzyme-related carboxypeptidase (ACE2) converts angiotensin I to angiotensin 1-9. Circ Res. 2000;87(5):E1-E9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
