

Congruence of opioid prescriptions and dispensing using electronic records and claims data
- PMID: 34008209
- PMCID: PMC8586485
- DOI: 10.1111/1475-6773.13673
Congruence of opioid prescriptions and dispensing using electronic records and claims data
Abstract
Objective: To quantify discrepancies between opioid prescribing and dispensing via the percentage of patients with Electronic Medical Record (EMR) prescriptions who subsequently filled the prescription within 90 days, defined as congruence, and compared opioid congruence with related medications.
Data sources: Deidentified data from the IBM MarketScan Explorys Claims-EMR Dataset.
Study design: In this retrospective, observational study, we examined congruence for commonly prescribed controlled substances-opioids, stimulants, and benzodiazepines. Congruence was stratified by age group and sex.
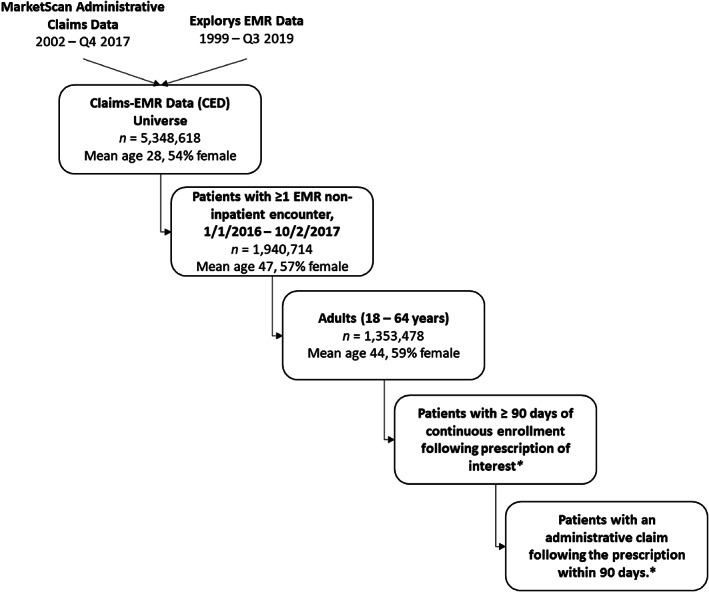
Data collection/extraction methods: Continuously enrolled adults aged 18-64 years with an EMR encounter (excluding inpatient settings) and ≥ 1 prescription for selected classes between 1/1/2016 and 10/2/2017.
Principal findings: During the study period, 1,353,478 adults had ≥1 EMR encounter. Patients with stimulants prescriptions had the highest congruence (83%) corresponding to 7151 claims for 8,635 EMR prescriptions, followed by opioids (66%; 62,766/95,690) and benzodiazepines (64%; 30,181/47,408). Chi-square testing showed congruence differed by age group within opioids (P < .0001) and benzodiazepines (P < .0001) and was higher among females within benzodiazepines (P < .0001).
Conclusions: These findings demonstrate that relying on claims data alone for opioid prescribing measures might underestimate actual prescribing magnitude by as much as one-third in these data. Combined EMR and claims data can help future research better understand characteristics associated with congruence or incongruence between prescribing and dispensing.
Keywords: benzodiazepines; claims; electronic medical records; prescription opioids; stimulants.
Published 2021. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures
Similar articles
-
Controlled Substance Prescribing Patterns--Prescription Behavior Surveillance System, Eight States, 2013.MMWR Surveill Summ. 2015 Oct 16;64(9):1-14. doi: 10.15585/mmwr.ss6409a1. MMWR Surveill Summ. 2015. PMID: 26469747
-
Mandatory Review of Prescription Drug Monitoring Program Before Issuance of a Controlled Substance Results in Overall Reduction of Prescriptions Including Opioids and Benzodiazepines.Pain Physician. 2020 Jun;23(3):299-304. Pain Physician. 2020. PMID: 32517396
-
Rates of Physician Coprescribing of Opioids and Benzodiazepines After the Release of the Centers for Disease Control and Prevention Guidelines in 2016.JAMA Netw Open. 2019 Aug 2;2(8):e198325. doi: 10.1001/jamanetworkopen.2019.8325. JAMA Netw Open. 2019. PMID: 31373650 Free PMC article.
-
Opioid Prescribing Patterns and Complications in the Dermatology Medicare Population.JAMA Dermatol. 2018 Mar 1;154(3):317-322. doi: 10.1001/jamadermatol.2017.5835. JAMA Dermatol. 2018. PMID: 29417134 Free PMC article.
-
Defining "Doctor Shopping" with Dispensing Data: A Scoping Review.Pain Med. 2022 Jul 1;23(7):1323-1332. doi: 10.1093/pm/pnab344. Pain Med. 2022. PMID: 34931686
Cited by
-
Concordance of opioid exposure in all-payer claims databases with prescription drug monitoring program database using Arkansas as a case example.Health Serv Res. 2023 Aug;58(4):938-947. doi: 10.1111/1475-6773.14117. Epub 2022 Dec 28. Health Serv Res. 2023. PMID: 36519709 Free PMC article.
References
-
- Hedegaard H, Miniño AM, Warner M. Drug overdose deaths in the United States, 1999‐2018. NCHS Data Brief. 2020;1–8. https://www.cdc.gov/nchs/data/databriefs/db356-h.pdf. - PubMed
-
- Baumblatt JAG, Wiedeman C, Dunn JR, Schaffner W, Paulozzi LJ, Jones TF. High‐risk use by patients prescribed opioids for pain and its role in overdose deaths. JAMA Intern Med. 2014;174(5):796‐801. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
