

Patient perceptions and use of non-statin lipid lowering therapy among patients with or at risk for atherosclerotic cardiovascular disease: Insights from the PALM registry
- PMID: 34008247
- PMCID: PMC8207979
- DOI: 10.1002/clc.23625
Patient perceptions and use of non-statin lipid lowering therapy among patients with or at risk for atherosclerotic cardiovascular disease: Insights from the PALM registry
Abstract
Background: Non-statin lipid lowering therapies (LLTs) provide additional treatment options for patients. Use patterns and patient perceptions of non-statin LLT remain incompletely described.
Hypothesis: The guideline-recommended statin intensity remains underutilized in patients treated with and without non-statin LLT.
Methods: The PALM Registry collected LLT information on patients with or at risk of ASCVD treated at 125 US clinics in 2015. We compared patient perceptions, lipid levels and statin use among patients treated with and without non-statin LLT.
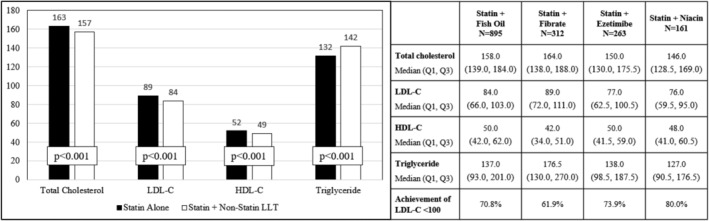
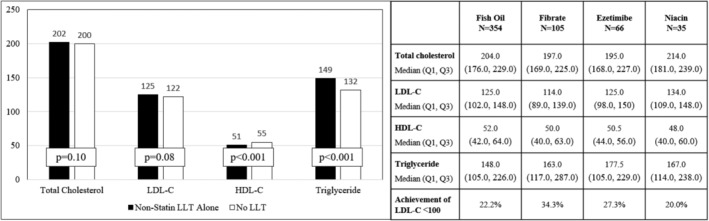
Results: Among 7720 patients, 1930 (25.0%) were treated with a non-statin LLT (1249 fish oil, 417 fibrates, 329 ezetimibe, 196 niacin). Concurrent statin treatment occurred in 73.7%, of which 45.4% were dosed under the guideline-recommended intensity. Compared with patients on statin alone, patients receiving both a statin and non-statin LLT (n = 1423) were more likely to be male, white race and to perceive themselves as higher risk of ASCVD compared with their peers (38.5% vs. 34.9%, p = .047). Only 27.4% of patients treated with non-statin LLT alone perceived themselves at higher risk. Most (75.7%) patients treated with a non-statin LLT alone reported never being treated with a statin, despite ASCVD in 30.8% of these patients. Among those previously treated with a statin, 59.3% reported being willing to try a statin again.
Conclusions: Non-statin LLT is used in one in four patients with or at risk for ASCVD; its use is frequently in place of statin therapy or in the absence of guideline-recommended statin intensity. More work is needed to establish statins as first line therapy.
Keywords: lipid-lowering therapy; primary prevention; secondary prevention; statin.
© 2021 The Authors. Clinical Cardiology published by Wiley Periodicals LLC.
Conflict of interest statement
Angela Lowenstern: Dr. Lowenstern reports funding through NIH T‐32 training grant #5 T32 HL069749‐14.
Shuang Li: Ms. Li reports no relevant disclosures.
Ann Marie Navar: Dr. Navar is supported by the NIH, NHLBI K01HL133416–01 and reports research support from Amgen, Sanofi, and Regeneron; consulting fees from Amgen and Sanofi.
Salim S. Virani: Dr. Virani reports research support from ADA/AHA/ VA; honorarium from ACC as the Associate Editor for Innovations,
Veronique L. Roger: Dr. Roger reports no relevant disclosures.
Jennifer G. Robinson: Dr. Robinson reports research support from Amarin, Amgen, Astra‐Zeneca, Eli Lilly, Esai, Glaxo‐Smith Kline, Merck, Pfizer, Regeneron/Sanofi, Takeda; consultant for Amgen, Eli Lilly, Merck, Pfizer, Regeneron/Sanofi.
Anne C. Goldberg: Dr. Goldberg reports research support from Amarin, Amgen, Pfizer, Merck, Regeneron/Sanofi, IONIS, Genzyme/Isis, and Regeneron, Madrigal, and Arisaph; consulting for Optum Rx, Regeneron/Sanofi, and Esperion; honorarium for editorial work Merck Manual.
Wendy Kampman: Dr. Kampman reports employment with Regeneron Pharmaceuticals, Inc.
Eric D. Peterson: Dr. Peterson reports research support from Eli Lilly, Janssen, Merck; Consulting from AstraZeneca, Bayer, Boehringer Ingelheim, Genentech, Janssen, Merck, and Sanofi Aventis.
Tracy Y. Wang: Dr. Wang reports research support from AstraZeneca, Daiichi Sankyo, Eli Lilly, Gilead, Glaxo SmithKline, Regeneron, Sanofi; consultant/advisory/education from Bristol Myers Squibb, Astra Zeneca, Eli Lilly, Premier, Inc.
Figures
Similar articles
-
Contemporary use of lipid-lowering therapy for secondary prevention in Korean patients with atherosclerotic cardiovascular diseases.Korean J Intern Med. 2020 May;35(3):593-604. doi: 10.3904/kjim.2018.312. Epub 2019 Nov 25. Korean J Intern Med. 2020. PMID: 31752475 Free PMC article.
-
Clinical characteristics and treatment patterns in patients with atherosclerotic cardiovascular disease with hypercholesterolemia: a retrospective analysis of a large US real-world database cohort.Curr Med Res Opin. 2024 Jan;40(1):15-25. doi: 10.1080/03007995.2023.2270901. Epub 2024 Jan 3. Curr Med Res Opin. 2024. PMID: 37941428
-
Variation in Lipid-Lowering Therapy Use in Patients With Low-Density Lipoprotein Cholesterol ≥190 mg/dL: Insights From the National Cardiovascular Data Registry-Practice Innovation and Clinical Excellence Registry.Circ Cardiovasc Qual Outcomes. 2018 May;11(5):e004652. doi: 10.1161/CIRCOUTCOMES.118.004652. Circ Cardiovasc Qual Outcomes. 2018. PMID: 29748356 Free PMC article.
-
More- Versus Less-Intensive Lipid-Lowering Therapy.Circ Cardiovasc Qual Outcomes. 2019 Aug;12(8):e005460. doi: 10.1161/CIRCOUTCOMES.118.005460. Epub 2019 Aug 15. Circ Cardiovasc Qual Outcomes. 2019. PMID: 31412729
-
Lipid management across Europe in the real-world setting: a rapid evidence review.Curr Med Res Opin. 2021 Dec;37(12):2049-2059. doi: 10.1080/03007995.2021.1973396. Epub 2021 Oct 12. Curr Med Res Opin. 2021. PMID: 34517739 Review.
Cited by
-
Lipid-lowering approaches to manage statin-intolerant patients.Eur Heart J Suppl. 2024 Apr 17;26(Suppl 1):i56-i59. doi: 10.1093/eurheartjsupp/suae007. eCollection 2024 Apr. Eur Heart J Suppl. 2024. PMID: 38867860 Free PMC article.
References
-
- Bittner V, Deng L, Rosenson RS, et al. Trends in the use of nonstatin lipid‐lowering therapy among patients with coronary heart disease: a retrospective cohort study in the Medicare population 2007 to 2011. J Am Coll Cardiol. 2015;66:1864‐1872. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129:S1‐S45. - PubMed
-
- Cannon CP, Blazing MA, Giugliano RP, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387‐2397. - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, et al. AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the Management of Blood Cholesterol. Circulation. 2018;2018:CIR0000000000000625. - PubMed
-
- Navar AM, Wang TY, Goldberg AC, et al. Design and rationale for the patient and provider assessment of lipid management (PALM) registry. Am Heart J. 2015;170:865‐871. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
