

doi: 10.36660/abc.20200422.
Dysautonomia: A Forgotten Condition - Part II
[Article in
English,
Portuguese]
Affiliations
- PMID: 34008826
- PMCID: PMC8121459
- DOI: 10.36660/abc.20200422
Item in Clipboard
Dysautonomia: A Forgotten Condition - Part II
[Article in
English,
Portuguese]
Arq Bras Cardiol.
2021 May.
No abstract available
Conflict of interest statement
Não há conflito com o presente artigo
Figures
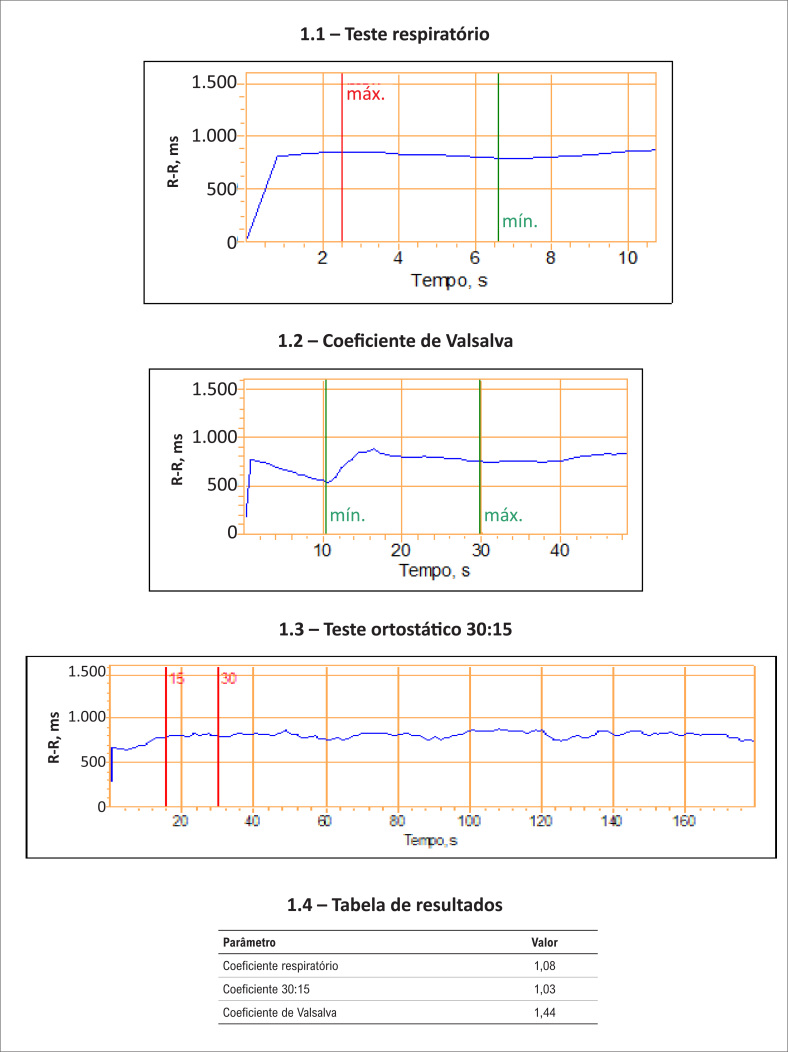
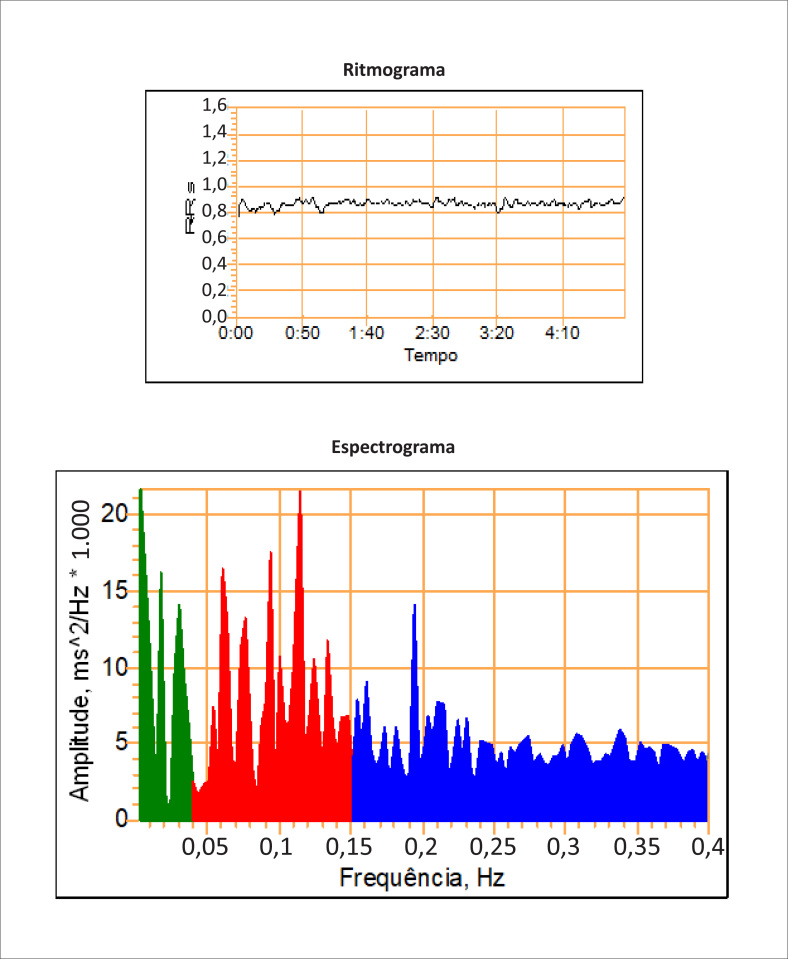
Componente de muito baixa frequência 0,01-0,04 Hz (FMB – VLF): avaliação das flutuações do tônus vasomotor ligado a termorregulação e a sudorese (ação predominante do simpático). Componente de baixa frequência 0,04-0,15 Hz (FB – LF): avaliação do barorreceptor (componente simpático predominante com modulação vagal). Componente de alta frequência 0,15-0,5 Hz (FA – HF): relacionado ao controle sinusal (ação parassimpática). Pode ser realizado no protocolo e em conjunto com os testes da Figura 1 (configurando o protocolo dos sete testes de avaliação dos reflexos autonômicos cardiovasculares).
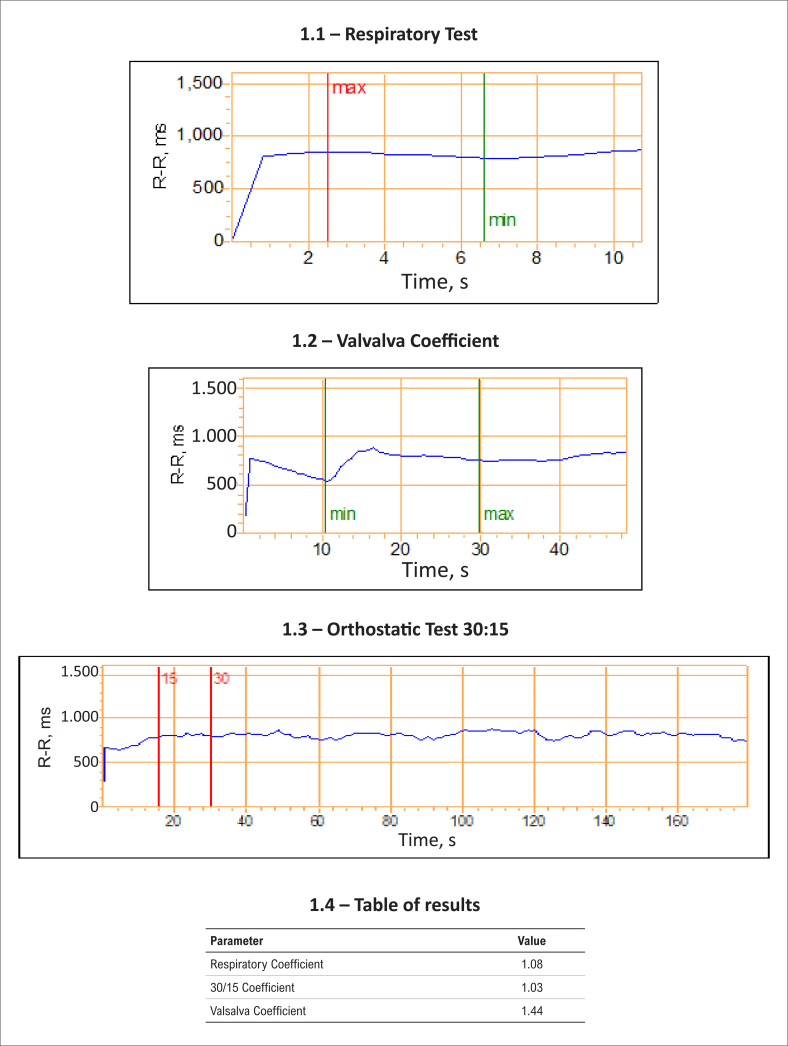
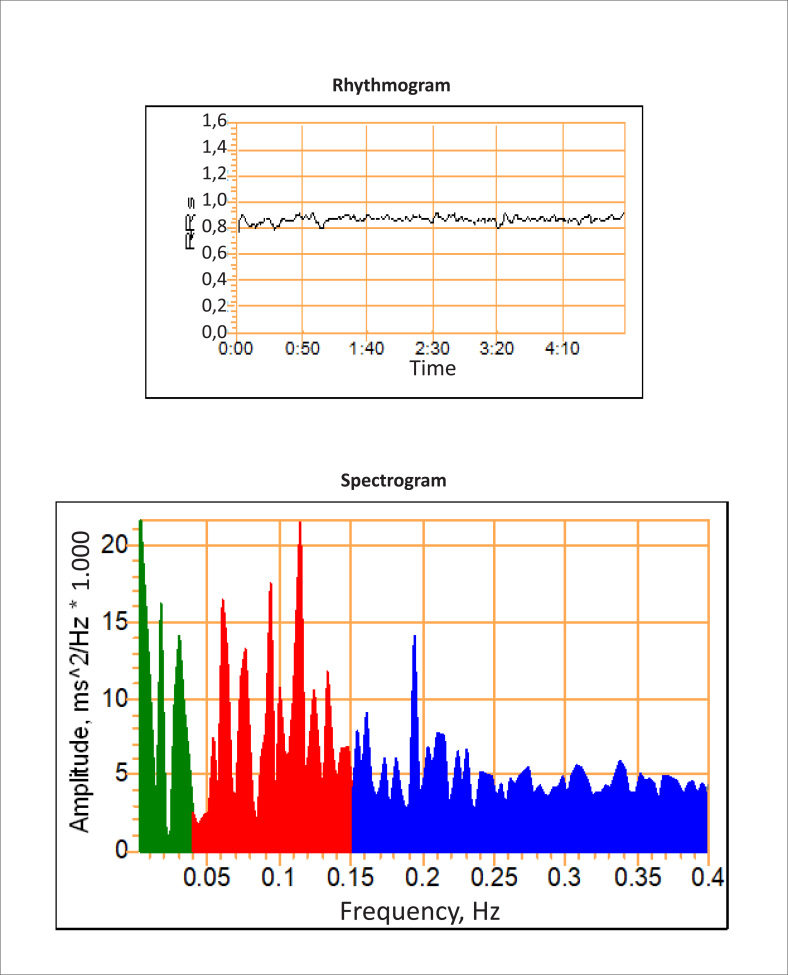
Very low frequency component — 0.01–0.04 Hz (FMB – VLF) — Assessment of vasomotor tone fluctuations related to thermoregulation and sweating — (predominant sympathetic action) Low Frequency Component — 0.04–0.15 Hz (FB-LF) — Baroreceptor evaluation (predominant sympathetic component with vagal modulation) High Frequency Component — 0.15–0.5 Hz (FA — HF) — Related to sinus control (parasympathetic action) It can be carried out in the protocol with the tests in
figure 1
(characterizing the protocol of the 7 Cardiovascular Autonomic Reflex Evaluation Tests).
Similar articles
-
ANA Investigates Dysautonomia.Ann Neurol. 2022 Jan;91(1):21-22. doi: 10.1002/ana.26273. Epub 2021 Nov 29. Ann Neurol. 2022. PMID: 34787333 No abstract available.
-
Dysautonomia after pediatric brain injury.Dev Med Child Neurol. 2012 Aug;54(8):683. doi: 10.1111/j.1469-8749.2012.04362.x. Epub 2012 Jun 19. Dev Med Child Neurol. 2012. PMID: 22712446 No abstract available.
-
Partial dysautonomia: An interesting presentation.Indian J Dermatol Venereol Leprol. 2017 Sep-Oct;83(5):596-598. doi: 10.4103/ijdvl.IJDVL_541_16. Indian J Dermatol Venereol Leprol. 2017. PMID: 28749384 No abstract available.
-
Calming the Storm: Dysautonomia for the Pediatrician.Curr Probl Pediatr Adolesc Health Care. 2017 Jul;47(7):145-150. doi: 10.1016/j.cppeds.2017.06.009. Epub 2017 Jul 15. Curr Probl Pediatr Adolesc Health Care. 2017. PMID: 28716515 Review.
-
Equine Dysautonomia.Vet Clin North Am Equine Pract. 2018 Apr;34(1):113-125. doi: 10.1016/j.cveq.2017.11.010. Epub 2018 Feb 3. Vet Clin North Am Equine Pract. 2018. PMID: 29398183 Review.
Cited by
-
Recurrent neurogenic shock as a rare postoperative complication associated with pancreaticoduodenectomy with mesopancreas excision in elderly patient: a case report.Gland Surg. 2024 Nov 30;13(11):2206-2211. doi: 10.21037/gs-23-494. Epub 2024 Nov 26. Gland Surg. 2024. PMID: 39678426 Free PMC article.
References
-
- 1. Rocha EA. Neurally mediated syndromes. Arq Brasil Cardiol. 2006; 87(3): e34-e44. - PubMed
-
- 2. Grubb BP, Olshanski B. Syncope: mechanisms and management. Armonk, NY: Futura Publishing Company; 1998: 107-26.
-
- 3. Lorga Filho AM, Magalhães LP, Cintra FD. Síncope. Rio de Janeiro: Atheneu. 2013. p. 35-52.
-
- 4. Shy GM, Drager GA. A neurological syndrome associated with orthostatic hypotension. Arch Neurol 1960; 2: 522-27. - PubMed
-
- 5. Quinn NP, Wenning G, Marsden CD. The shy-drager syndrome. What did shy and drager really describe? Arch Neurol. 1995; 52(7): 656-7. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
