

Abundance of P-glycoprotein and Breast Cancer Resistance Protein Measured by Targeted Proteomics in Human Epileptogenic Brain Tissue
- PMID: 34008992
- PMCID: PMC8488956
- DOI: 10.1021/acs.molpharmaceut.1c00083
Abundance of P-glycoprotein and Breast Cancer Resistance Protein Measured by Targeted Proteomics in Human Epileptogenic Brain Tissue
Abstract
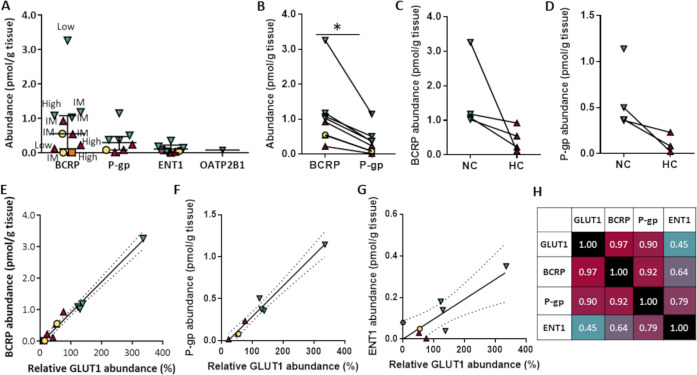
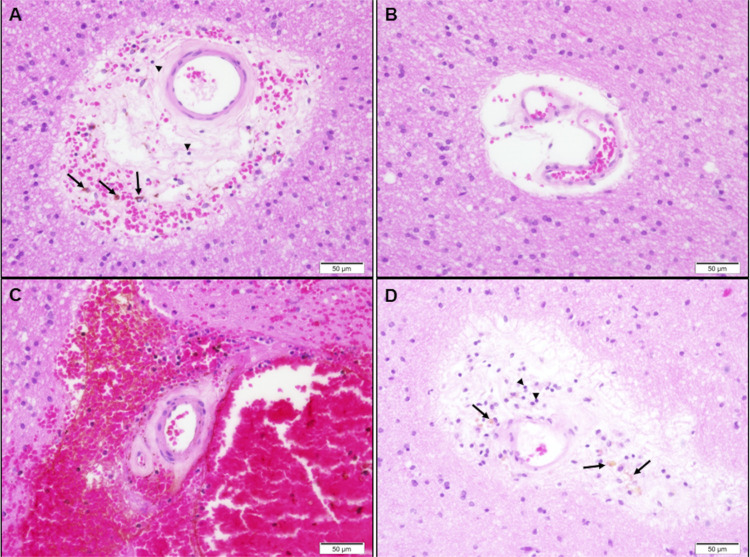
Our goal was to measure the absolute differential abundance of key drug transporters in human epileptogenic brain tissue and to compare them between patients and at various distances from the epileptogenic zone within the same patient. Transporter protein abundance was quantified in brain tissue homogenates from patients who underwent epilepsy surgery, using targeted proteomics, and correlations with clinical and tissue characteristics were assessed. Fourteen brain samples (including four epileptogenic hippocampal samples) were collected from nine patients. Among the quantifiable drug transporters, the abundance (median, range) ranked: breast cancer resistance protein (ABCG2/BCRP; 0.55, 0.01-3.26 pmol/g tissue) > P-glycoprotein (ABCB1/MDR1; 0.30, 0.02-1.15 pmol/g tissue) > equilibrative nucleoside transporter 1 (SLC29A1/ENT1; 0.06, 0.001-0.35 pmol/g tissue). The ABCB1/ABCG2 ratio (mean 0.27, range 0.08-0.47) was comparable with literature values from nonepileptogenic brain tissue (mean 0.5-0.8). Transporter abundance was lower in the hippocampi than in the less epileptogenic neocortex of the same patients. ABCG2/BCRP and ABCB1/MDR1 expression strongly correlated with that of glucose transporter 1 (SLC2A1/GLUT1) (r = 0.97, p < 0.001; r = 0.90, p < 0.01, respectively). Low transporter abundance was found in patients with overt vascular pathology, whereas the highest abundance was seen in a sample with normally appearing blood vessels. In conclusion, drug transporter abundance highly varies across patients and between epileptogenic and less epileptogenic brain tissue of the same patient. The strong correlation in abundance of ABCB1/MDR1, ABCG2/BCRP, and SLC2A1/GLUT1 suggests variation in the content of the functional vasculature within the tissue samples. The epileptogenic tissue can be depleted of key drug transport mechanisms, warranting consideration when selecting treatments for patients with drug-resistant epilepsy.
Keywords: P-glycoprotein; antiepileptic drugs; antiseizure medications; breast cancer resistance protein; epilepsy; targeted proteomics.
Conflict of interest statement
The authors declare the following competing financial interest(s): Sara Eyal has received speaker honoraria from Megapharm, Israel. The remaining authors have no conflicts of interest.
Figures
References
-
- Kwan P.; Arzimanoglou A.; Berg A. T.; Brodie M. J.; Allen Hauser W.; Mathern G.; et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 2010, 51, 1069–1077. 10.1111/j.1528-1167.2009.02397.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
