

A pilot study to assess the circulating renin-angiotensin system in COVID-19 acute respiratory failure
- PMID: 34009036
- PMCID: PMC8270515
- DOI: 10.1152/ajplung.00129.2021
A pilot study to assess the circulating renin-angiotensin system in COVID-19 acute respiratory failure
Abstract
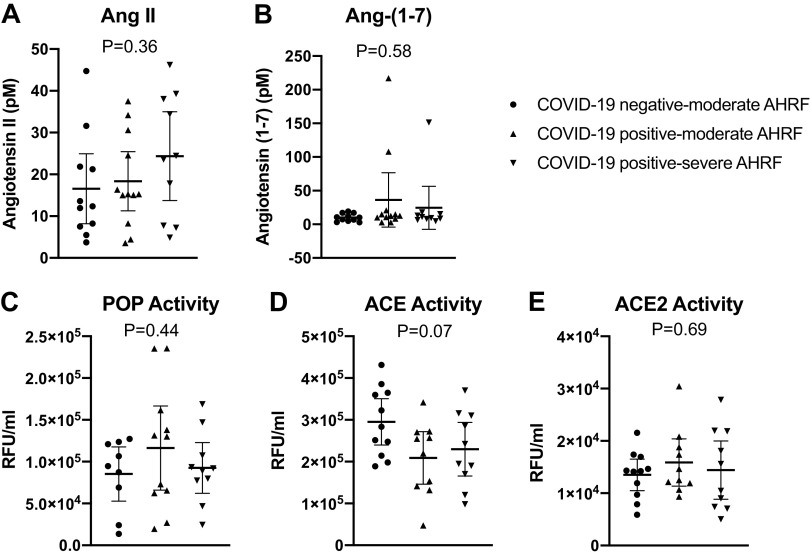
The renin-angiotensin system (RAS) is fundamental to COVID-19 pathobiology, due to the interaction between the SARS-CoV-2 virus and the angiotensin-converting enzyme 2 (ACE2) coreceptor for cellular entry. The prevailing hypothesis is that SARS-CoV-2-ACE2 interactions lead to an imbalance of the RAS, favoring proinflammatory angiotensin II (ANG II)-related signaling at the expense of the anti-inflammatory ANG-(1-7)-mediated alternative pathway. Indeed, multiple clinical trials targeting this pathway in COVID-19 are underway. Therefore, precise measurement of circulating RAS components is critical to understand the interplay of the RAS on COVID-19 outcomes. Multiple challenges exist in measuring the RAS in COVID-19, including improper patient controls, ex vivo degradation and low concentrations of angiotensins, and unvalidated laboratory assays. Here, we conducted a prospective pilot study to enroll 33 patients with moderate and severe COVID-19 and physiologically matched COVID-19-negative controls to quantify the circulating RAS. Our enrollment strategy led to physiological matching of COVID-19-negative and COVID-19-positive moderate hypoxic respiratory failure cohorts, in contrast to the severe COVID-19 cohort, which had increased severity of illness, prolonged intensive care unit (ICU) stay, and increased mortality. Circulating ANG II and ANG-(1-7) levels were measured in the low picomolar (pM) range. We found no significant differences in circulating RAS peptides or peptidases between these three cohorts. The combined moderate and severe COVID-19-positive cohorts demonstrated a mild reduction in ACE activity compared with COVID-19-negative controls (2.2 ± 0.9 × 105 vs. 2.9 ± 0.8 × 105 RFU/mL, P = 0.03). These methods may be useful in designing larger studies to physiologically match patients and quantify the RAS in COVID-19 RAS augmenting clinical trials.
Keywords: ACE2; SARS-CoV-2; acute respiratory distress syndrome; angiotensin; critical care.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures

Similar articles
-
The circulating renin-angiotensin system and mortality among patients hospitalized for COVID-19: a mechanistic substudy of the ACTIV-4 Host Tissue trials.Am J Physiol Lung Cell Mol Physiol. 2025 Mar 1;328(3):L405-L412. doi: 10.1152/ajplung.00372.2024. Epub 2025 Jan 30. Am J Physiol Lung Cell Mol Physiol. 2025. PMID: 39884670 Free PMC article.
-
Dysregulation of ACE (Angiotensin-Converting Enzyme)-2 and Renin-Angiotensin Peptides in SARS-CoV-2 Mediated Mortality and End-Organ Injuries.Hypertension. 2022 Feb;79(2):365-378. doi: 10.1161/HYPERTENSIONAHA.121.18295. Epub 2021 Nov 30. Hypertension. 2022. PMID: 34844421
-
Expression of ACE2, Soluble ACE2, Angiotensin I, Angiotensin II and Angiotensin-(1-7) Is Modulated in COVID-19 Patients.Front Immunol. 2021 Jun 14;12:625732. doi: 10.3389/fimmu.2021.625732. eCollection 2021. Front Immunol. 2021. PMID: 34194422 Free PMC article.
-
The fight against COVID-19: Striking a balance in the renin-angiotensin system.Drug Discov Today. 2021 Oct;26(10):2214-2220. doi: 10.1016/j.drudis.2021.04.006. Epub 2021 Apr 15. Drug Discov Today. 2021. PMID: 33865979 Free PMC article. Review.
-
Disequilibrium between the classic renin-angiotensin system and its opposing arm in SARS-CoV-2-related lung injury.Am J Physiol Lung Cell Mol Physiol. 2020 Aug 1;319(2):L325-L336. doi: 10.1152/ajplung.00189.2020. Epub 2020 Jul 8. Am J Physiol Lung Cell Mol Physiol. 2020. PMID: 32639866 Free PMC article. Review.
Cited by
-
The Renin-Angiotensin System (RAS) in COVID-19 Disease: Where We Are 3 Years after the Beginning of the Pandemic.Microorganisms. 2024 Mar 14;12(3):583. doi: 10.3390/microorganisms12030583. Microorganisms. 2024. PMID: 38543635 Free PMC article. Review.
-
The systemic renin-angiotensin system in COVID-19.Sci Rep. 2022 Nov 22;12(1):20117. doi: 10.1038/s41598-022-24628-1. Sci Rep. 2022. PMID: 36418458 Free PMC article.
-
The Renin-Angiotensin-Aldosterone System in COVID-19-related and Non-COVID-19-related Acute Respiratory Distress Syndrome: Not So Different after All?Am J Respir Crit Care Med. 2021 Nov 1;204(9):1007-1008. doi: 10.1164/rccm.202108-1904ED. Am J Respir Crit Care Med. 2021. PMID: 34473935 Free PMC article. No abstract available.
-
Repressed Ang 1-7 in COVID-19 Is Inversely Associated with Inflammation and Coagulation.mSphere. 2022 Aug 31;7(4):e0022022. doi: 10.1128/msphere.00220-22. Epub 2022 Aug 1. mSphere. 2022. PMID: 35913134 Free PMC article.
-
Plasmatic renin-angiotensin system in normotensive and hypertensive patients hospitalized with COVID-19.Biomed Pharmacother. 2022 Aug;152:113201. doi: 10.1016/j.biopha.2022.113201. Epub 2022 May 27. Biomed Pharmacother. 2022. PMID: 35661534 Free PMC article.
References
-
- Sparks MA, South AM, Badley AD, Baker-Smith CM, Batlle D, Bozkurt B, Cattaneo R, Crowley SD, Dell'Italia LJ, Ford AL, Griendling K, Gurley SB, Kasner SE, Murray JA, Nath KA, Pfeffer MA, Rangaswami J, Taylor WR, Garovic VD. Severe acute respiratory syndrome coronavirus 2, COVID-19, and the renin-angiotensin system: pressing needs and best research practices. Hypertension 76: 1350–1367, 2020. doi:10.1161/HYPERTENSIONAHA.120.15948. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous