

Optimization of duplex velocity criteria for diagnosis of internal carotid artery (ICA) stenosis: A report of the Intersocietal Accreditation Commission (IAC) Vascular Testing Division Carotid Diagnostic Criteria Committee
- PMID: 34009060
- PMCID: PMC8493430
- DOI: 10.1177/1358863X211011253
Optimization of duplex velocity criteria for diagnosis of internal carotid artery (ICA) stenosis: A report of the Intersocietal Accreditation Commission (IAC) Vascular Testing Division Carotid Diagnostic Criteria Committee
Abstract
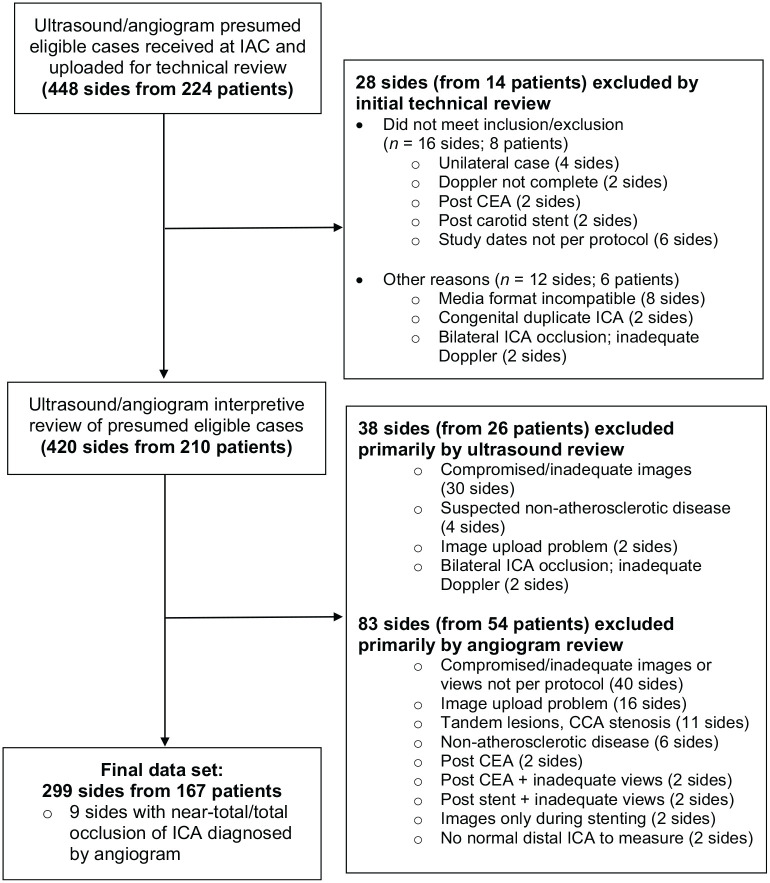
Diagnostic criteria to classify severity of internal carotid artery (ICA) stenosis vary across vascular laboratories. Consensus-based criteria, proposed by the Society of Radiologists in Ultrasound in 2003 (SRUCC), have been broadly implemented but have not been adequately validated. We conducted a multicentered, retrospective correlative imaging study of duplex ultrasound versus catheter angiography for evaluation of severity of ICA stenosis. Velocity data were abstracted from bilateral duplex studies performed between 1/1/2009 and 12/31/2015 and studies were interpreted using SRUCC. Percentage ICA stenosis was determined using North American Symptomatic Carotid Endarterectomy Trial (NASCET) methodology. Receiver operating characteristic analysis evaluated the performance of SRUCC parameters compared with angiography. Of 448 ICA sides (from 224 patients), 299 ICA sides (from 167 patients) were included. Agreement between duplex ultrasound and angiography was moderate (κ = 0.42), with overestimation of degree of stenosis for both moderate (50-69%) and severe (⩾ 70%) ICA lesions. The primary SRUCC parameter for ⩾ 50% ICA stenosis of peak-systolic velocity (PSV) of ⩾ 125 cm/sec did not meet prespecified thresholds for adequate sensitivity, specificity, and accuracy (sensitivity 97.8%, specificity 64.2%, accuracy 74.5%). Test performance was improved by raising the PSV threshold to ⩾ 180 cm/sec (sensitivity 93.3%, specificity 81.6%, accuracy 85.2%) or by adding the additional parameter of ICA/common carotid artery (CCA) PSV ratio ⩾ 2.0 (sensitivity 94.3%, specificity 84.3%, accuracy 87.4%). For ⩾ 70% ICA stenosis, analysis was limited by a low number of cases with angiographically severe disease. Interpretation of carotid duplex examinations using SRUCC resulted in significant overestimation of severity of ICA stenosis when compared with angiography; raising the PSV threshold for ⩾ 50% ICA stenosis to ⩾ 180 cm/sec as a single parameter or requiring the ICA/CCA PSV ratio ⩾ 2.0 in addition to PSV of ⩾ 125 cm/sec for laboratories using the SRUCC is recommended to improve the accuracy of carotid duplex examinations.
Keywords: carotid artery disease; carotid duplex ultrasound; diagnostic criteria; vascular imaging/diagnostics.
Conflict of interest statement
Figures
References
-
- Brott TG, Halperin JL, Abbara S, et al. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. Circulation 2011; 124: e54–130. - PubMed
-
- Fell G, Phillips DJ, Chikos PM, et al. Ultrasonic duplex scanning for disease of the carotid artery. Circulation 1981; 64: 1191–1195. - PubMed
-
- Taylor DC, Strandness DE., Jr. Carotid artery duplex scanning. J Clin Ultrasound 1987; 15: 635–644. - PubMed
-
- Moneta GL, Edwards JM, Chitwood RW, et al. Correlation of North American Symptomatic Carotid Endarterectomy Trial (NASCET) angiographic definition of 70% to 99% internal carotid artery stenosis with duplex scanning. J Vasc Surg 1993; 17: 152–157; discussion 157–159. - PubMed
-
- Bluth EI, Stavros AT, Marich KW, et al. Carotid duplex sonography: A multicenter recommendation for standardized imaging and Doppler criteria. Radiographics 1988; 8: 487–506. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
