

Evaluation of the Risk of Stroke Without Anticoagulation Therapy in Men and Women With Atrial Fibrillation Aged 66 to 74 Years Without Other CHA2DS2-VASc Factors
- PMID: 34009232
- PMCID: PMC8135054
- DOI: 10.1001/jamacardio.2021.1232
Evaluation of the Risk of Stroke Without Anticoagulation Therapy in Men and Women With Atrial Fibrillation Aged 66 to 74 Years Without Other CHA2DS2-VASc Factors
Abstract
Importance: There are limited clinical trial data and discrepant recommendations regarding use of anticoagulation therapy in patients with atrial fibrillation (AF) aged 65 to 74 years without other stroke risk factors.
Objectives: To evaluate the risk of stroke without anticoagulation therapy in men and women with AF aged 66 to 74 years without other CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years, diabetes, stroke, vascular disease, age 65-74 years, female sex) risk factors and examine the association of stroke incidence with patient age.
Design, setting, and participants: A population-based retrospective cohort study was conducted using linked administrative databases. The population included 16 351 individuals aged 66 to 74 years who were newly diagnosed with AF in Ontario, Canada, between April 1, 2007, and March 31, 2017. Exclusion criteria included long-term care residence, prior anticoagulation therapy, valvular disease, heart failure, hypertension, diabetes, stroke, and vascular disease. The cumulative incidence function was used to estimate the 1-year incidence of stroke in patients who did not receive anticoagulation therapy. Fine-Gray regression was used to study the association of patient characteristics with stroke incidence and derive estimates of stroke risk at each age. Death was treated as a competing risk and patients were censored if they initiated anticoagulation therapy. Inverse probability of censoring weights was used to account for patient censoring. Data analysis was performed from May 26, 2019, to December 9, 2020.
Exposures: Atrial fibrillation and age.
Main outcomes and measures: Hospitalizations for stroke.
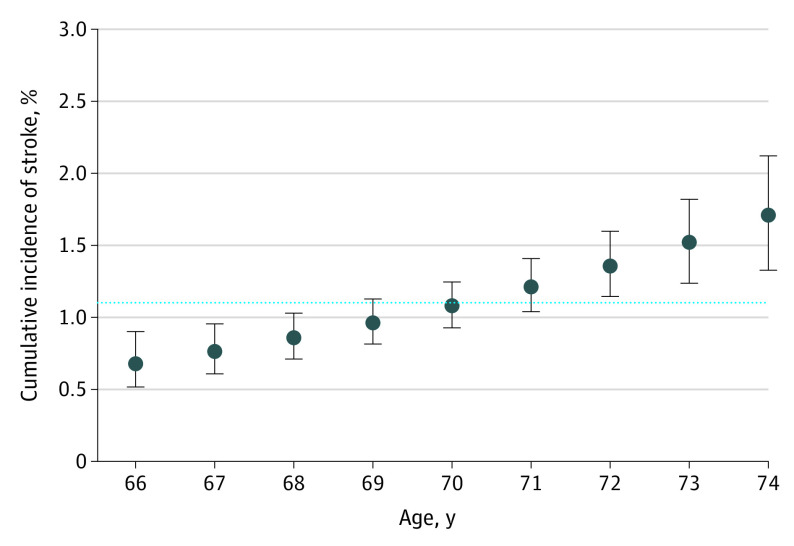
Results: Of the 16 351 individuals with AF (median [interquartile range] age, 70 [68-72] years), 8352 (51.1%) were men; 6314 individuals (38.6%) started anticoagulation therapy during follow-up. The overall 1-year stroke incidence among patients who did not receive anticoagulation therapy was 1.1% (95% CI, 1.0%-1.3%) and the incidence of death without stroke was 8.1% (95% CI, 7.7%-8.5%). The incidence of stroke was not significantly associated with sex. The estimated 1-year stroke risk increased with patient age from 66 years (0.7%; 95% CI, 0.5%-0.9%) to 74 years (1.7%; 95% CI, 1.3%-2.1%).
Conclusions and relevance: The risk of stroke more than doubled in this study as men and women with AF but no other CHA2DS2-VASc risk factors aged from 66 to 74 years. These data suggest that anticoagulation therapy is more likely to benefit older individuals within this group of patients, whereas younger individuals are less likely to gain net clinical benefit from anticoagulation therapy.
Conflict of interest statement
Figures

Comment in
-
Competing Risks, Treatment Switching, and Informative Censoring.JAMA Cardiol. 2021 Aug 1;6(8):871-873. doi: 10.1001/jamacardio.2021.1239. JAMA Cardiol. 2021. PMID: 34009256 No abstract available.
References
-
- Lip GY, Nieuwlaat R, Pisters R, Lane DA, Crijns HJ. Refining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillation. Chest. 2010;137(2):263-272. doi: 10.1378/chest.09-1584 - DOI - PubMed
-
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125-e151. doi: 10.1161/CIR.0000000000000665 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
