

Association of Socioeconomic Disadvantage With Long-term Mortality After Myocardial Infarction: The Mass General Brigham YOUNG-MI Registry
- PMID: 34009238
- PMCID: PMC8135064
- DOI: 10.1001/jamacardio.2021.0487
Association of Socioeconomic Disadvantage With Long-term Mortality After Myocardial Infarction: The Mass General Brigham YOUNG-MI Registry
Abstract
Importance: Socioeconomic disadvantage is associated with poor health outcomes. However, whether socioeconomic factors are associated with post-myocardial infarction (MI) outcomes in younger patient populations is unknown.
Objective: To evaluate the association of neighborhood-level socioeconomic disadvantage with long-term outcomes among patients who experienced an MI at a young age.
Design, setting, and participants: This cohort study analyzed patients in the Mass General Brigham YOUNG-MI Registry (at Brigham and Women's Hospital and Massachusetts General Hospital in Boston, Massachusetts) who experienced an MI at or before 50 years of age between January 1, 2000, and April 30, 2016. Each patient's home address was mapped to the Area Deprivation Index (ADI) to capture higher rates of socioeconomic disadvantage. The median follow-up duration was 11.3 years. The dates of analysis were May 1, 2020, to June 30, 2020.
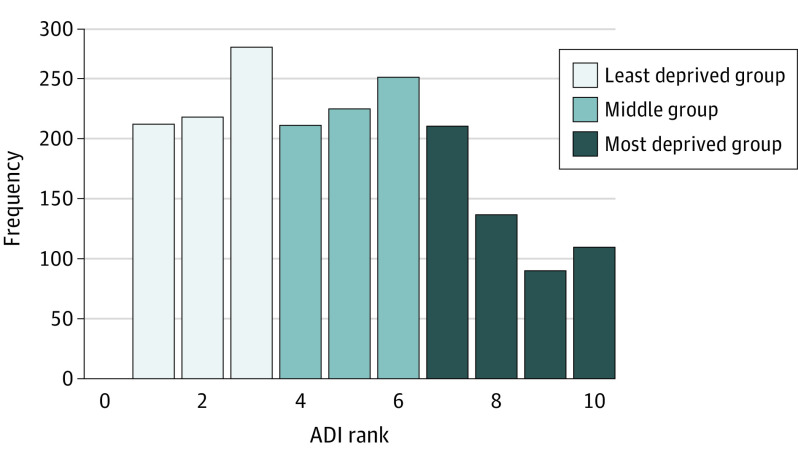
Exposures: Patients were assigned an ADI ranking according to their home address and then stratified into 3 groups (least disadvantaged group, middle group, and most disadvantaged group).
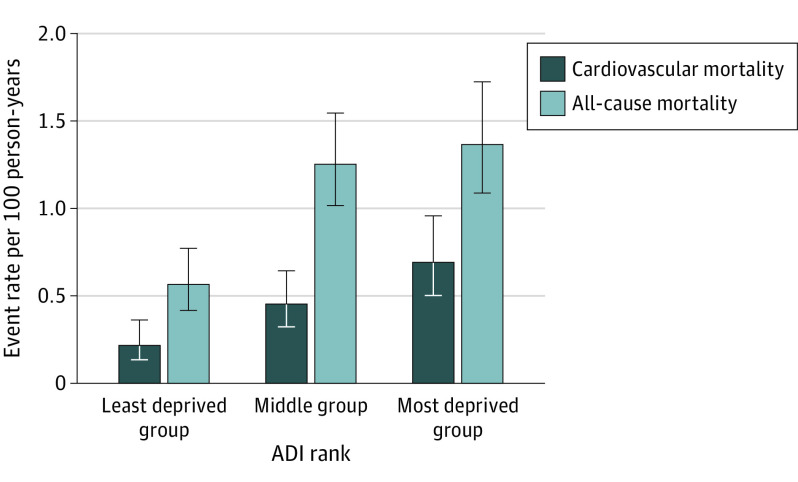
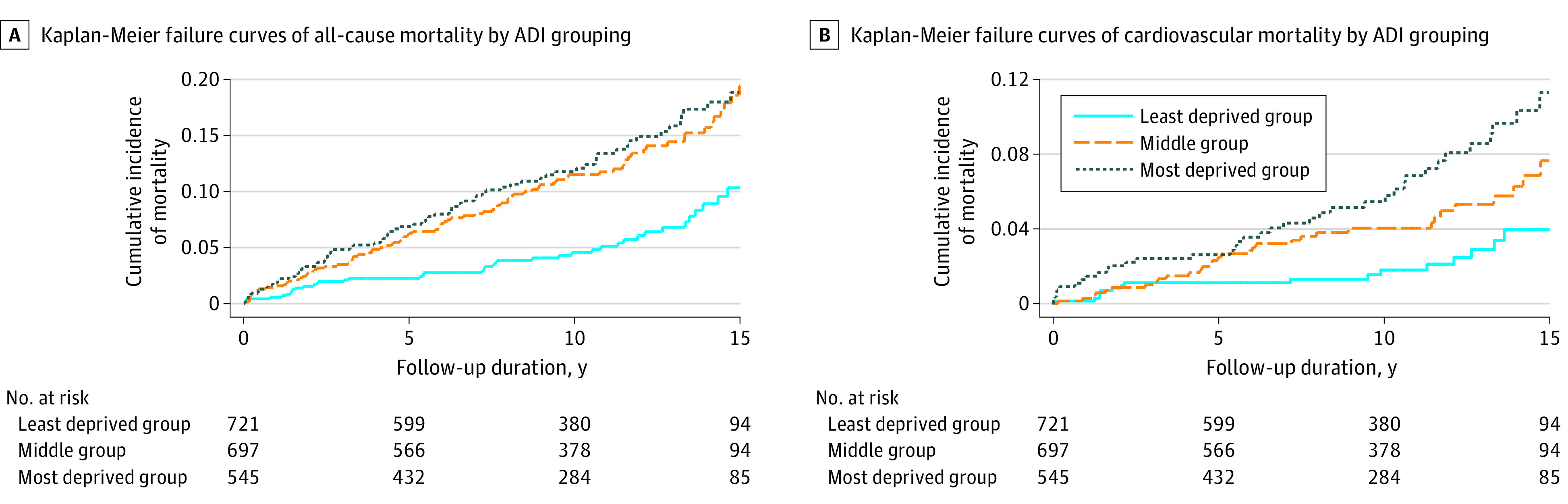
Main outcomes and measures: The outcomes of interest were all-cause and cardiovascular mortality. Cause of death was adjudicated from national registries and electronic medical records. Cox proportional hazards regression modeling was used to evaluate the association of ADI with all-cause and cardiovascular mortality.
Results: The cohort consisted of 2097 patients, of whom 2002 (95.5%) with an ADI ranking were included (median [interquartile range] age, 45 [42-48] years; 1607 male individuals [80.3%]). Patients in the most disadvantaged neighborhoods were more likely to be Black or Hispanic, have public insurance or no insurance, and have higher rates of traditional cardiovascular risk factors such as hypertension and diabetes. Among the 1964 patients who survived to hospital discharge, 74 (13.6%) in the most disadvantaged group compared with 88 (12.6%) in the middle group and 41 (5.7%) in the least disadvantaged group died. Even after adjusting for a comprehensive set of clinical covariates, higher neighborhood disadvantage was associated with a 32% higher all-cause mortality (hazard ratio, 1.32; 95% CI, 1.10-1.60; P = .004) and a 57% higher cardiovascular mortality (hazard ratio, 1.57; 95% CI, 1.17-2.10; P = .003).
Conclusions and relevance: This study found that, among patients who experienced an MI at or before age 50 years, socioeconomic disadvantage was associated with higher all-cause and cardiovascular mortality even after adjusting for clinical comorbidities. These findings suggest that neighborhood and socioeconomic factors have an important role in long-term post-MI survival.
Conflict of interest statement
Figures
Comment in
-
Does Health Inequity Begin at Home?JAMA Cardiol. 2021 Aug 1;6(8):889-890. doi: 10.1001/jamacardio.2021.0500. JAMA Cardiol. 2021. PMID: 34009237 No abstract available.
-
Role of Income-Lifting Social Programs in Reducing Years of Life Lost to Myocardial Infarction and Sudden Death-Reply.JAMA Cardiol. 2022 Feb 1;7(2):230-231. doi: 10.1001/jamacardio.2021.5130. JAMA Cardiol. 2022. PMID: 34910076 No abstract available.
-
Role of Income-Lifting Social Programs in Reducing Years of Life Lost to Myocardial Infarction and Sudden Death.JAMA Cardiol. 2022 Feb 1;7(2):230. doi: 10.1001/jamacardio.2021.5127. JAMA Cardiol. 2022. PMID: 34910079 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
