

Triple vs Dual Inhaler Therapy and Asthma Outcomes in Moderate to Severe Asthma: A Systematic Review and Meta-analysis
- PMID: 34009257
- PMCID: PMC8135065
- DOI: 10.1001/jama.2021.7872
Triple vs Dual Inhaler Therapy and Asthma Outcomes in Moderate to Severe Asthma: A Systematic Review and Meta-analysis
Abstract
Importance: The benefits and harms of adding long-acting muscarinic antagonists (LAMAs) to inhaled corticosteroids (ICS) and long-acting β2-agonists (LABAs) for moderate to severe asthma remain unclear.
Objective: To systematically synthesize the outcomes and adverse events associated with triple therapy (ICS, LABA, and LAMA) vs dual therapy (ICS plus LABA) in children and adults with persistent uncontrolled asthma.
Data sources: MEDLINE, Embase, CENTRAL, ICTRP, FDA, and EMA databases from November 2017, to December 8, 2020, without language restriction.
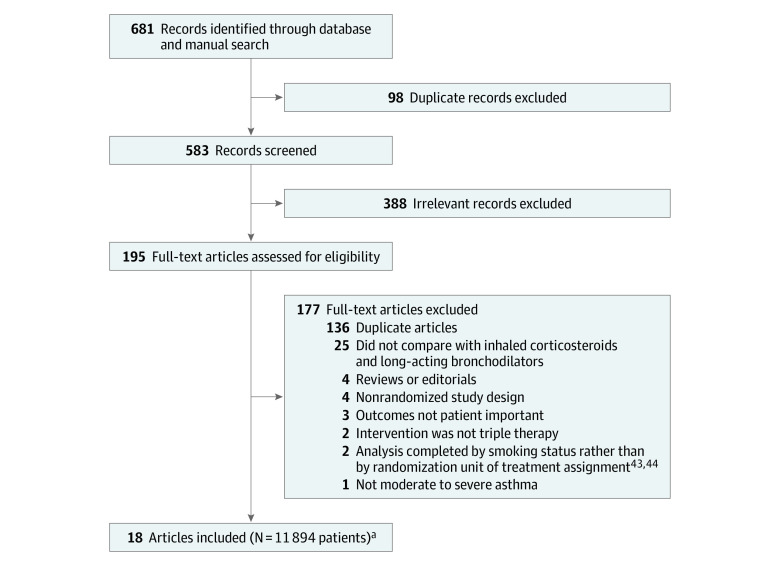
Study selection: Two investigators independently selected randomized clinical trials (RCTs) comparing triple vs dual therapy in patients with moderate to severe asthma.
Data extraction and synthesis: Two reviewers independently extracted data and assessed risk of bias. Random-effects meta-analyses, including individual patient-level exacerbation data, were used. The GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach was used to assess certainty (quality) of the evidence.
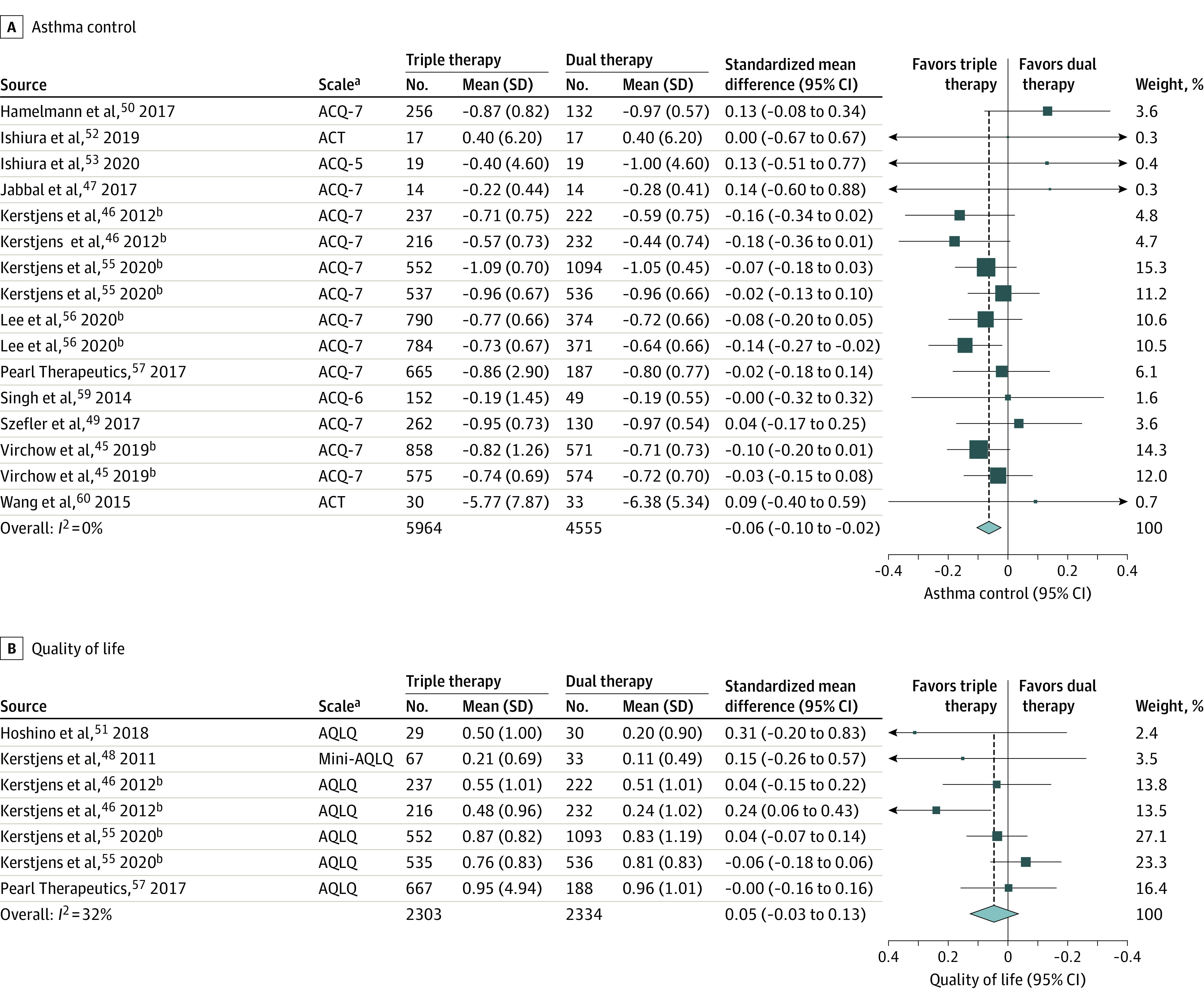
Main outcomes and measures: Severe exacerbations, asthma control (measured using the Asthma Control Questionnaire [ACQ-7], a 7-item list with each item ranging from 0 [totally controlled] to 6 [severely uncontrolled]; minimal important difference, 0.5), quality of life (measured using the Asthma-related Quality of Life [AQLQ] tool; score range, 1 [severely impaired] to 7 [no impairment]; minimal important difference, 0.5), mortality, and adverse events.
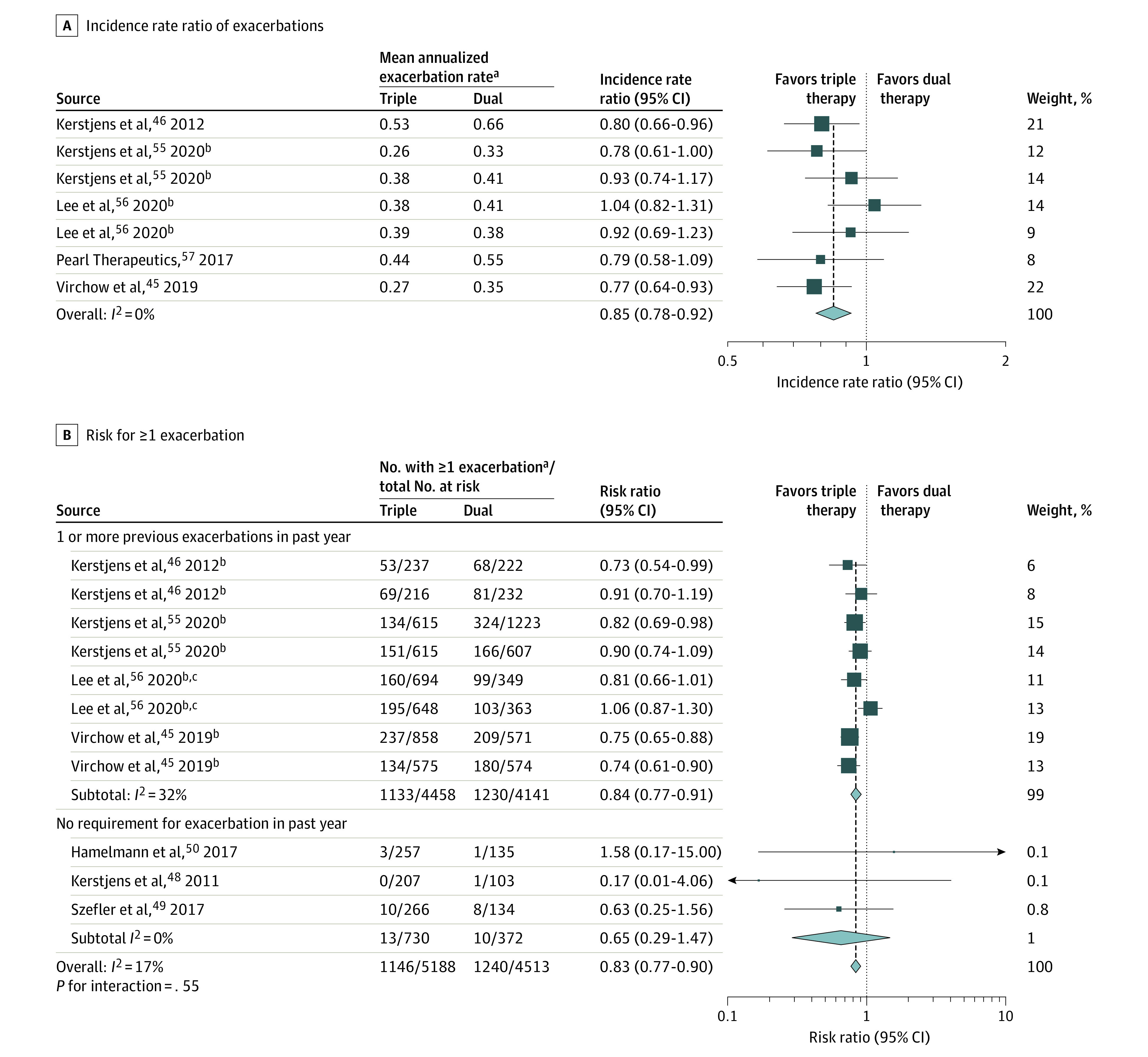
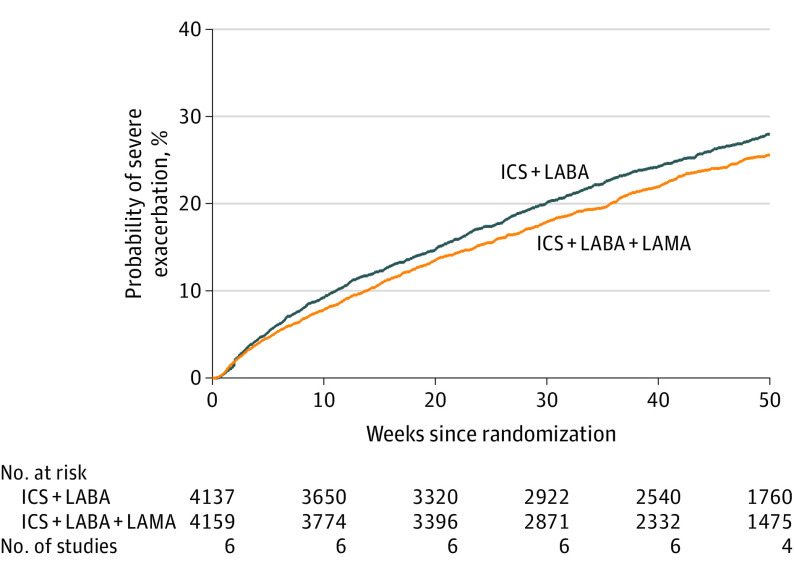
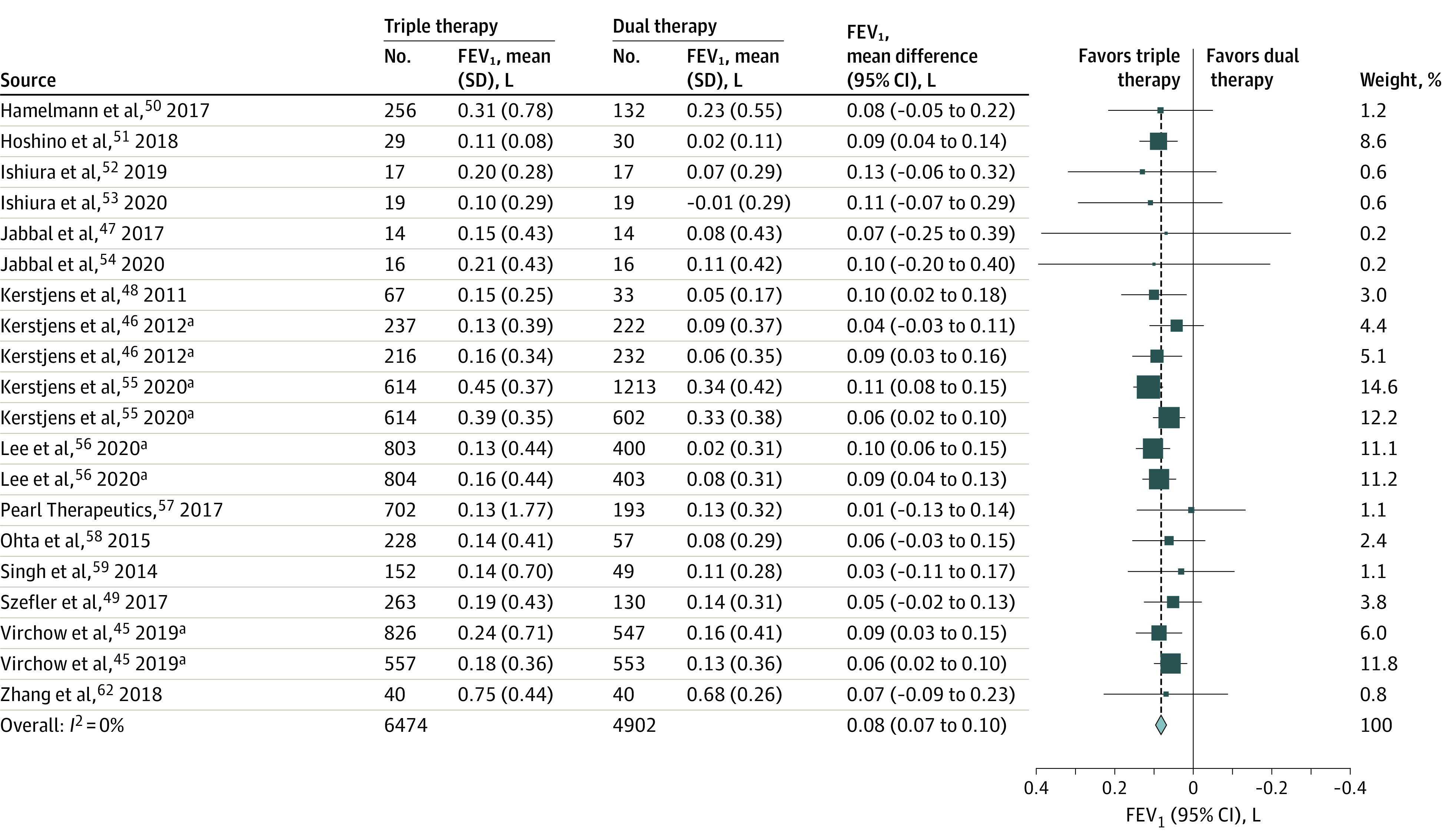
Results: Twenty RCTs using 3 LAMA types that enrolled 11 894 children and adults (mean age, 52 years [range, 9-71 years]; 57.7% female) were included. High-certainty evidence showed that triple therapy vs dual therapy was significantly associated with a reduction in severe exacerbation risk (9 trials [9932 patients]; 22.7% vs 27.4%; risk ratio, 0.83 [95% CI, 0.77 to 0.90]) and an improvement in asthma control (14 trials [11 230 patients]; standardized mean difference [SMD], -0.06 [95% CI, -0.10 to -0.02]; mean difference in ACQ-7 scale, -0.04 [95% CI, -0.07 to -0.01]). There were no significant differences in asthma-related quality of life (7 trials [5247 patients]; SMD, 0.05 [95% CI, -0.03 to 0.13]; mean difference in AQLQ score, 0.05 [95% CI, -0.03 to 0.13]; moderate-certainty evidence) or mortality (17 trials [11 595 patients]; 0.12% vs 0.12%; risk ratio, 0.96 [95% CI, 0.33 to 2.75]; high-certainty evidence) between dual and triple therapy. Triple therapy was significantly associated with increased dry mouth and dysphonia (10 trials [7395 patients]; 3.0% vs 1.8%; risk ratio, 1.65 [95% CI, 1.14 to 2.38]; high-certainty evidence), but treatment-related and serious adverse events were not significantly different between groups (moderate-certainty evidence).
Conclusions and relevance: Among children (aged 6 to 18 years) and adults with moderate to severe asthma, triple therapy, compared with dual therapy, was significantly associated with fewer severe asthma exacerbations and modest improvements in asthma control without significant differences in quality of life or mortality.
Conflict of interest statement
Figures
Comment in
-
Dual vs. Triple Therapy for Patients with Moderate to Severe Asthma.Am J Nurs. 2021 Sep 1;121(9):56. doi: 10.1097/01.NAJ.0000790636.32742.fc. Am J Nurs. 2021. PMID: 34438430
References
-
- Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2020 update. Accessed December 16, 2020. https://ginasthma.org
-
- Cloutier MM, Baptist AP, Blake KV, et al. ; Expert Panel Working Group of the National Heart, Lung, and Blood Institute . 2020 Focused updates to the asthma management guidelines: a report from the National Asthma Education and Prevention Program Coordinating Committee Expert Panel Working Group. J Allergy Clin Immunol. 2020;146(6):1217-1270. doi:10.1016/j.jaci.2020.10.003 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
