

Afirma Genomic Sequencing Classifier and Xpression Atlas Molecular Findings in Consecutive Bethesda III-VI Thyroid Nodules
- PMID: 34009369
- PMCID: PMC8277199
- DOI: 10.1210/clinem/dgab304
Afirma Genomic Sequencing Classifier and Xpression Atlas Molecular Findings in Consecutive Bethesda III-VI Thyroid Nodules
Abstract
Context: Broad genomic analyses among thyroid histologies have been described from relatively small cohorts.
Objective: Investigate the molecular findings across a large, real-world cohort of thyroid fine-needle aspiration (FNA) samples.
Design: Retrospective analysis of RNA sequencing data files.
Setting: Clinical Laboratory Improvement Amendments laboratory performing Afirma Genomic Sequencing Classifier (GSC) and Xpression Atlas (XA) testing.
Participants: A total of 50 644 consecutive Bethesda III-VI nodules.
Intervention: None.
Main outcome measures: Molecular test results.
Results: Of 48 952 Bethesda III/IV FNAs studied, 66% were benign by Afirma GSC. The prevalence of BRAF V600E was 2% among all Bethesda III/IV FNAs and 76% among Bethesda VI FNAs. Fusions involving NTRK, RET, BRAF, and ALK were most prevalent in Bethesda V (10%), and 130 different gene partners were identified. Among small consecutive Bethesda III/IV sample cohorts with one of these fusions and available surgical pathology excision data, the positive predictive value of an NTRK or RET fusion for carcinoma or noninvasive follicular thyroid neoplasm with papillary-like nuclear features was >95%, whereas for BRAF and ALK fusions it was 81% and 67%, respectively. At least 1 genomic alteration was identified by the expanded Afirma XA panel in 70% of medullary thyroid carcinoma classifier-positive FNAs, 44% of Bethesda III or IV Afirma GSC suspicious FNAs, 64% of Bethesda V FNAs, and 87% of Bethesda VI FNAs.
Conclusions: This large study demonstrates that almost one-half of Bethesda III/IV Afirma GSC suspicious and most Bethesda V/VI nodules had at least 1 genomic variant or fusion identified, which may optimize personalized treatment decisions.
Keywords: indeterminate cytology; molecular diagnostics; personalized healthcare; thyroid cancer; thyroid nodule; variant detection.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
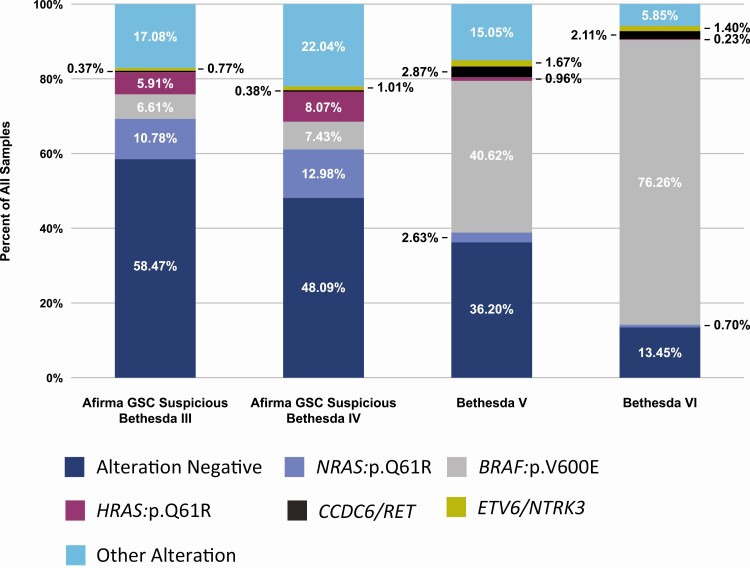
 = Alteration Negative;
= Alteration Negative;  = NRAS:p.Q61R;
= NRAS:p.Q61R;  = BRAF:p.V600E;
= BRAF:p.V600E;  = HRAS:p.Q61R;
= HRAS:p.Q61R;  = CCDC6/RET;
= CCDC6/RET;  = ETV6/NTRK3;
= ETV6/NTRK3;  = Other Alteration.
= Other Alteration.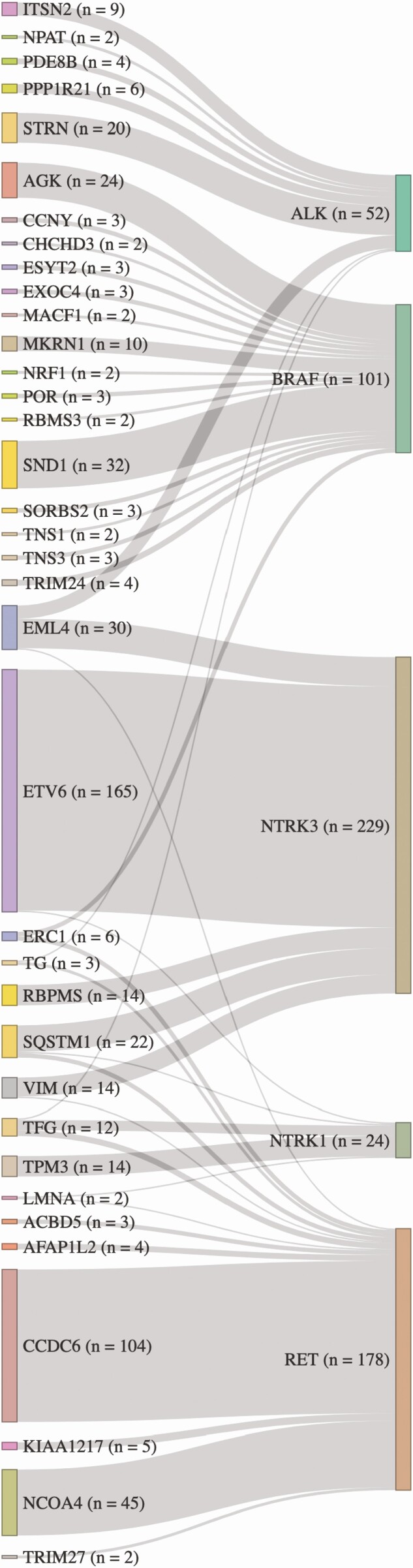
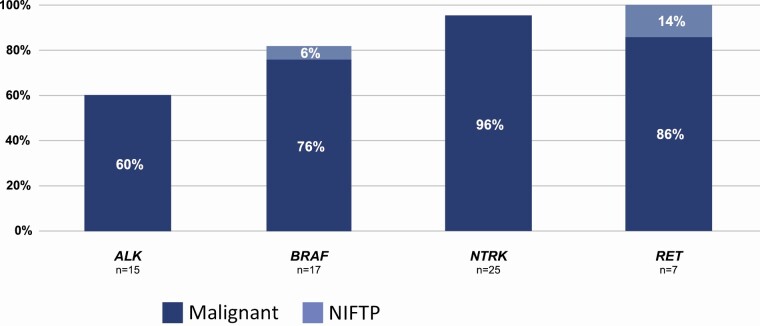
 = Malignant;
= Malignant;  = NIFTP.
= NIFTP.
Comment in
-
Indeterminate Thyroid Nodules: The Hazy Genomic Landscape Coming into Focus.J Clin Endocrinol Metab. 2021 Oct 21;106(11):e4781-e4783. doi: 10.1210/clinem/dgab441. J Clin Endocrinol Metab. 2021. PMID: 34139768 No abstract available.
References
-
- American Thyroid Association Guidelines Taskforce on Thyroid N, Differentiated Thyroid C, Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167-1214. - PubMed
-
- Patel KN, Yip L, Lubitz CC, et al. The American Association of Endocrine Surgeons guidelines for the definitive surgical management of thyroid disease in adults. Annals of surgery. 2020;271(3):e21-e93. - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology. Thyroid carcinoma. NCCN Clinical Practice Guidelines in Oncology. National Comprehensive Cancer Network; 2021. Version 1.2021.
-
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1-133. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
