

Clinical implication of quantitative flow ratio to predict clinical events after drug-coated balloon angioplasty in patients with in-stent restenosis
- PMID: 34009672
- PMCID: PMC8259159
- DOI: 10.1002/clc.23630
Clinical implication of quantitative flow ratio to predict clinical events after drug-coated balloon angioplasty in patients with in-stent restenosis
Abstract
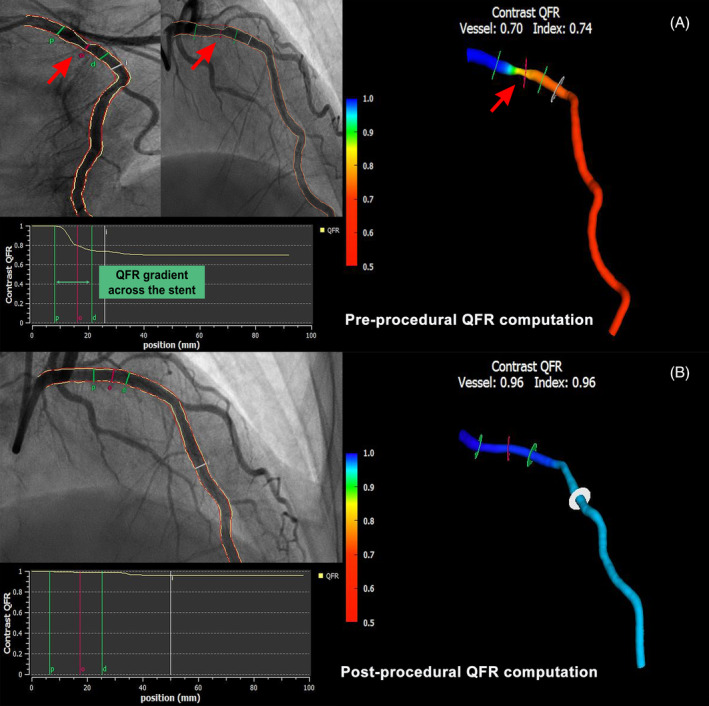
Background: The association between the quantitative flow ratio (QFR) and adverse events after drug-coated balloon (DCB) angioplasty for in-stent restenosis (ISR) lesions has not been investigated.
Hypothesis: Post-procedural QFR is related to adverse events in patients undergoing DCB angioplasty for ISR lesions.
Methods: This retrospective study included data from patients undergoing DCB angioplasty for drug-eluting stent (DES) ISR between January 2016 and February 2019. The QFR was measured at baseline and after DCB angioplasty. The endpoint was the vessel-oriented composite endpoint (VOCE), defined as a composite of cardiac death, vessel-related myocardial infarction, and ischemia-driven target vessel revascularization.
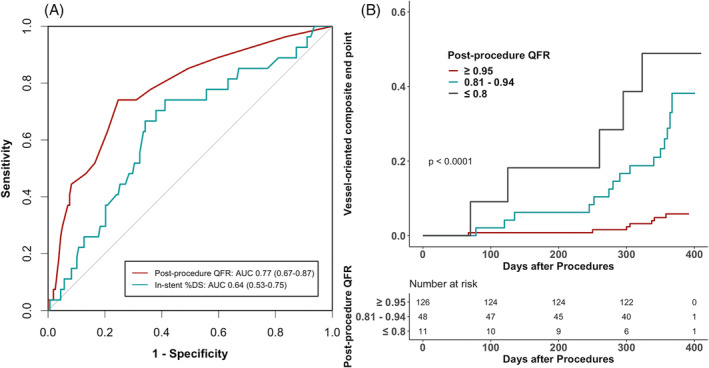
Results: Overall, 177 patients with 185 DES-ISR lesions were included. During 1-year follow-up, 27 VOCEs occurred in 26 patients. The area under curve (AUC) of the post-procedural QFR was statistically greater than that of the in-stent percent diameter stenosis (0.77, 95% confidence interval [CI] 0.67-0.87 vs. 0.64, 95% CI 0.53-0.75; p = .032). Final QFR cutoff of 0.94 has the best predictive accuracy for VOCE. A QFR > 0.94 was associated with a lower risk of VOCE compared to a QFR ≤ 0.94 (log-rank test, p < .0001). Survival analysis using the multivariable Cox model showed that a post-procedural QFR ≤ 0.94 was an independent predictor of 1-year VOCE (hazard ratio 6.53, 95% CI 2.70-15.8, p < .001).
Conclusions: A lower QFR value was associated with worse clinical outcomes at 1 year after DCB angioplasty for DES-ISR.
Keywords: drug-coated balloon; percutaneous coronary intervention; quantitative flow ratio.
© 2021 The Authors. Clinical Cardiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors have no potential conflict of interest.
Figures
Similar articles
-
Clinical Value of the Quantitative Flow Ratio to Predict Long-term Target Vessel Failure in Patients with In-stent Restenosis after Drug-coated Balloon Angioplasty.Curr Med Sci. 2024 Jun;44(3):561-567. doi: 10.1007/s11596-024-2876-0. Epub 2024 May 29. Curr Med Sci. 2024. PMID: 38809380
-
Prognostic value of post-procedural μQFR for drug-coated balloons in the treatment of in-stent restenosis.Cardiol J. 2023;30(2):167-177. doi: 10.5603/CJ.a2021.0154. Epub 2021 Nov 23. Cardiol J. 2023. PMID: 34811717 Free PMC article.
-
Comparison between drug-coated balloon angioplasty and second-generation drug-eluting stent placement for the treatment of in-stent restenosis after drug-eluting stent implantation.Heart Vessels. 2016 Sep;31(9):1405-11. doi: 10.1007/s00380-015-0741-6. Epub 2015 Sep 4. Heart Vessels. 2016. PMID: 26337620
-
Long-term clinical safety and efficacy of drug-coated balloon in the treatment of in-stent restenosis: A meta-analysis and systematic review.Catheter Cardiovasc Interv. 2020 Aug;96(2):E129-E141. doi: 10.1002/ccd.28572. Epub 2019 Nov 12. Catheter Cardiovasc Interv. 2020. PMID: 31714010
-
Second-generation drug-eluting stents versus drug-coated balloons for the treatment of coronary in-stent restenosis: A systematic review and meta-analysis.Catheter Cardiovasc Interv. 2018 Aug 1;92(2):285-299. doi: 10.1002/ccd.27359. Epub 2017 Oct 10. Catheter Cardiovasc Interv. 2018. PMID: 29024274
Cited by
-
Clinical Value of the Quantitative Flow Ratio to Predict Long-term Target Vessel Failure in Patients with In-stent Restenosis after Drug-coated Balloon Angioplasty.Curr Med Sci. 2024 Jun;44(3):561-567. doi: 10.1007/s11596-024-2876-0. Epub 2024 May 29. Curr Med Sci. 2024. PMID: 38809380
-
Illusion of revascularization: does anyone achieve optimal revascularization during percutaneous coronary intervention?Nat Rev Cardiol. 2024 Sep;21(9):652-662. doi: 10.1038/s41569-024-01014-0. Epub 2024 May 7. Nat Rev Cardiol. 2024. PMID: 38710772 Review.
-
Intravascular Ultrasound-Based Fractional Flow Reserve for Predicting Prognosis after Percutaneous Coronary Intervention.J Cardiovasc Transl Res. 2023 Dec;16(6):1417-1424. doi: 10.1007/s12265-023-10409-2. Epub 2023 Jul 13. J Cardiovasc Transl Res. 2023. PMID: 37440164
-
A 2024 scientific update on the clinical performance of drug-coated balloons.AsiaIntervention. 2024 Feb 29;10(1):15-25. doi: 10.4244/AIJ-D-23-00010. eCollection 2024 Feb. AsiaIntervention. 2024. PMID: 38425817 Free PMC article. Review.
-
Angiography-based Fractional Flow Reserve for the Prediction of Clinical Outcomes After Drug-coated Balloon or Plain Old Balloon Angioplasty.Cardiovasc Drugs Ther. 2025 Aug;39(4):791-800. doi: 10.1007/s10557-024-07575-z. Epub 2024 May 28. Cardiovasc Drugs Ther. 2025. PMID: 38805160
References
-
- Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus‐ and paclitaxel‐eluting coronary stents. N Engl J Med. 2007;356:998‐1008. - PubMed
-
- Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus‐eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346:1773‐1780. - PubMed
-
- Alfonso F, Byrne RA, Rivero F, Kastrati A. Current treatment of in‐stent restenosis. J Am Coll Cardiol. 2014;63:2659‐2673. - PubMed
-
- Alfonso F, Scheller B. State of the art: balloon catheter technologies‐drug‐coated balloon. EuroIntervention. 2017;13:680‐695. - PubMed
-
- Haybar H, Shahrabi S, Rezaeeyan H, Shirzad R, Saki N. Endothelial cells: from dysfunction mechanism to pharmacological effect in cardiovascular disease. Cardiovasc Toxicol. 2019;19:13‐22. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
