

Dizziness, Psychosocial Function, and Postural Stability Following Sport-Related Concussion
- PMID: 34009789
- PMCID: PMC8426409
- DOI: 10.1097/JSM.0000000000000923
Dizziness, Psychosocial Function, and Postural Stability Following Sport-Related Concussion
Abstract
Objective: To examine if self-reported dizziness is associated with concussion symptoms, depression and/or anxiety symptoms, or gait performance within 2 weeks of postconcussion.
Design: Cross-sectional study.
Setting: Research laboratory.
Participants: Participants were diagnosed with a concussion within 14 days of initial testing (N = 40). Participants were divided into 2 groups based on their Dizziness Handicap Inventory (DHI) score: 36 to 100 = moderate/severe dizziness and 0 to 35 = mild/no dizziness.
Interventions: Participants were tested on a single occasion and completed the DHI, hospital anxiety and depression scale (HADS), Patient Health Questionnaire-9 (PHQ-9), and Post-Concussion Symptom Inventory (PCSI). Three different postural control tests were use: modified Balance Error Scoring System, single-/dual-task tandem gait, and a single-/dual-task instrumented steady-state gait analysis.
Main outcome measures: Comparison of patient-reported outcomes and postural control outcomes between moderate/severe (DHI ≥ 36) and mild/no (DHI < 36) dizziness groups.
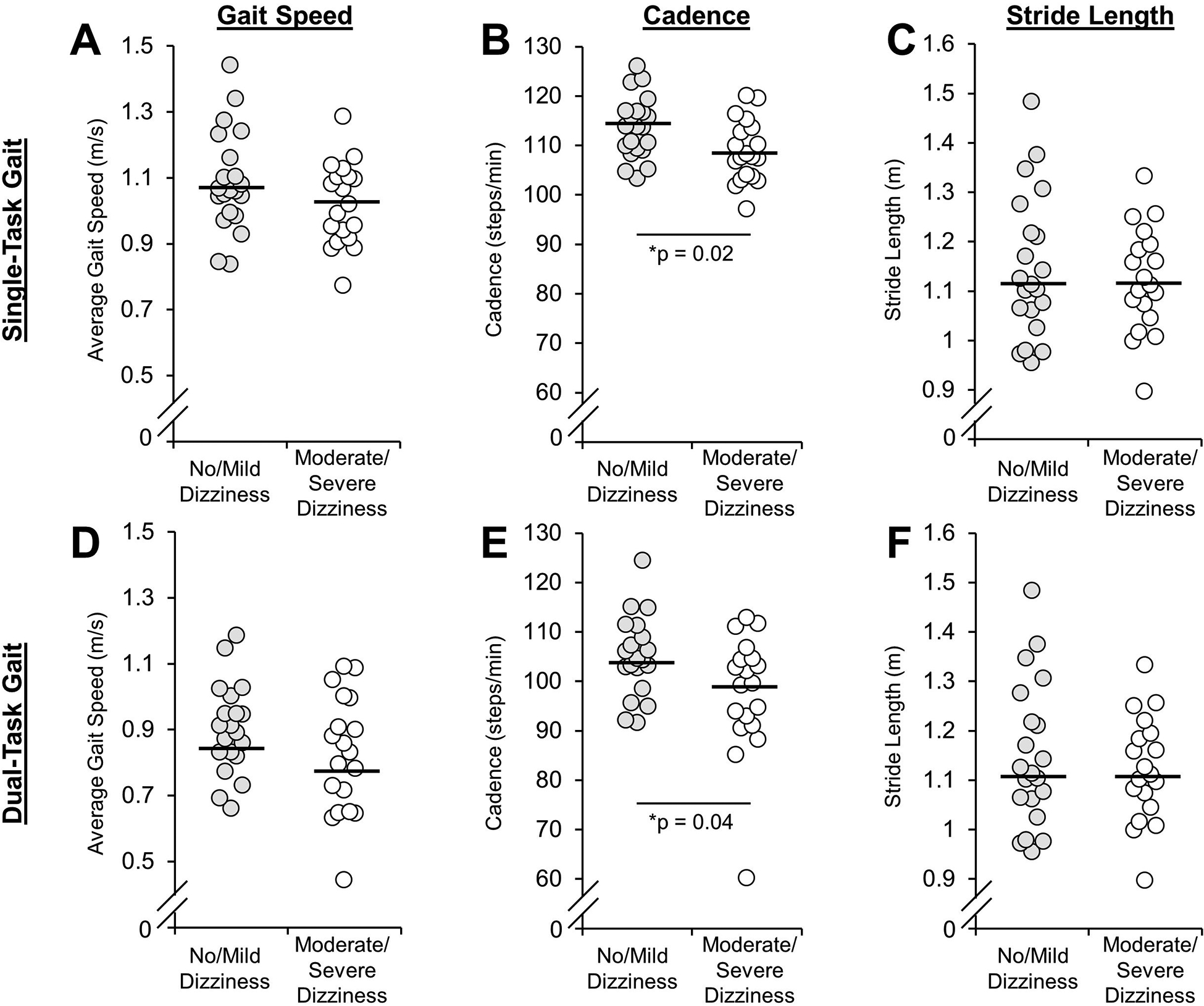
Results: Participants with moderate/severe dizziness (n = 19; age = 17.1 ± 2.4 years; 63% female) reported significantly higher symptom burden (PSCI: 43.0 ± 20.6 vs 22.8 ± 15.7; P = 0.001) and had higher median HADS anxiety (6 vs 2; P < 0.001) and depression (6 vs 1; P = 0.001) symptom severity than those with no/minimal dizziness (n = 21; age = 16.5 ± 1.9; 38% female). During steady-state gait, moderate/severe dizziness group walked with significantly slower single-task cadence (mean difference = 4.8 steps/minute; 95% confidence interval = 0.8, 8.8; P = 0.02) and dual-task cadence (mean difference = 7.4 steps/minute; 95% confidence interval = 0.7, 14.0; P = 0.04) than no/mild dizziness group.
Conclusion: Participants who reported moderate/severe dizziness reported higher concussion symptom burden, higher anxiety scores, and higher depression scores than those with no/mild dizziness. Cadence during gait was also associated with the level of dizziness reported.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Conflicts of interest
Unrelated to this study, Dr. Howell has received research support from the National Institute of Neurological Disorders And Stroke (R01NS100952 and R43NS108823) and MINDSOURCE Brain Injury Network. Dr. Meehan receives royalties from 1) ABC-Clio publishing for the sale of his books,
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
