

Final Report of a Trial of Intensive versus Standard Blood-Pressure Control
- PMID: 34010531
- PMCID: PMC9907774
- DOI: 10.1056/NEJMoa1901281
Final Report of a Trial of Intensive versus Standard Blood-Pressure Control
Abstract
Background: In a previously reported randomized trial of standard and intensive systolic blood-pressure control, data on some outcome events had yet to be adjudicated and post-trial follow-up data had not yet been collected.
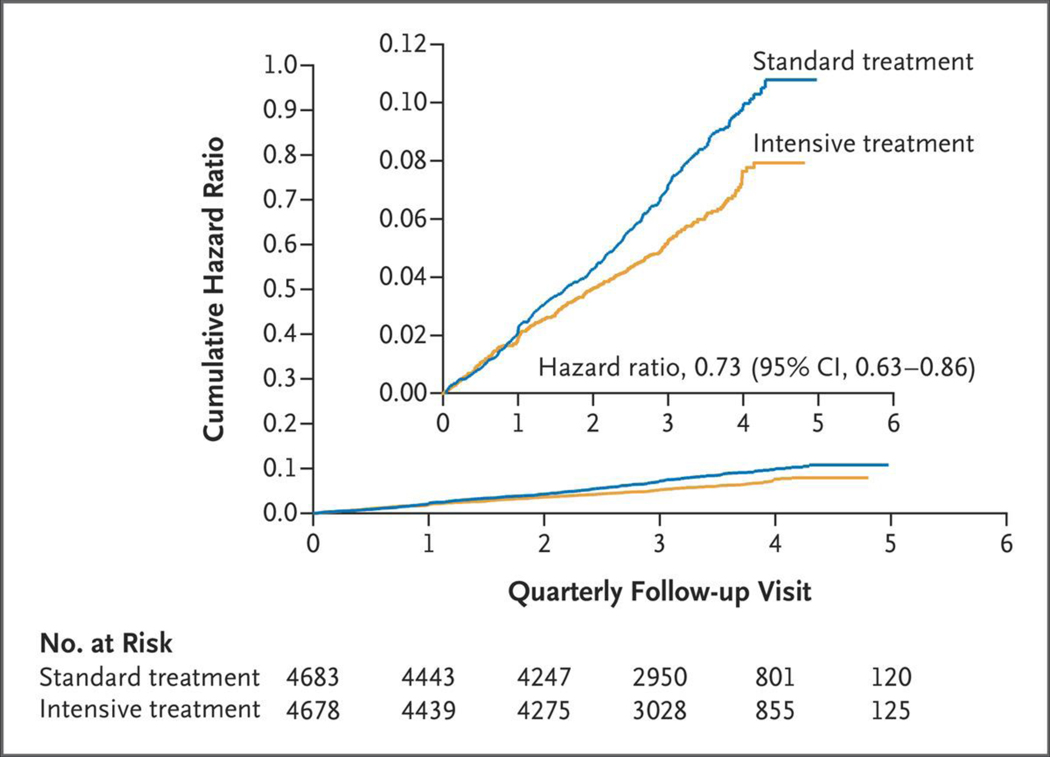
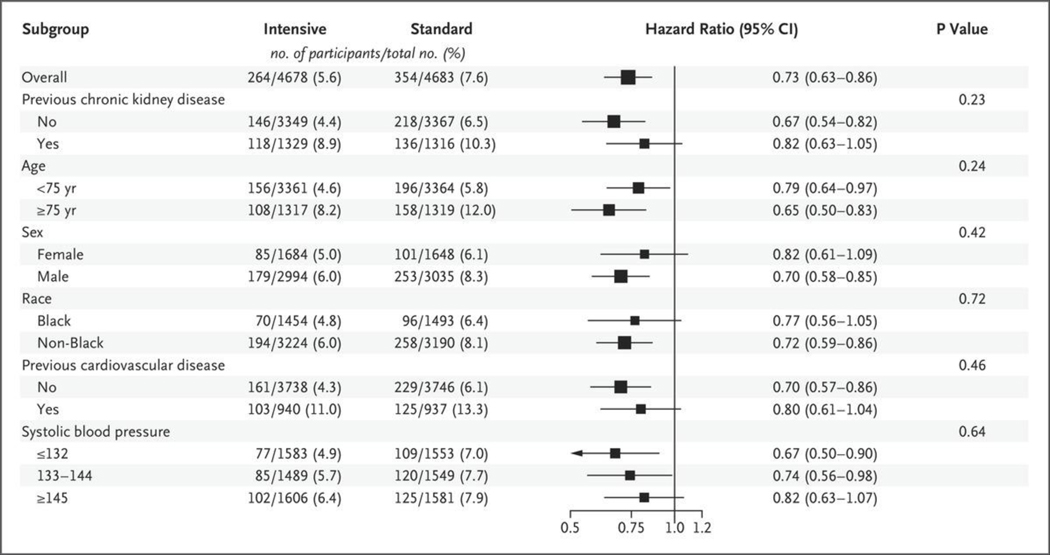
Methods: We randomly assigned 9361 participants who were at increased risk for cardiovascular disease but did not have diabetes or previous stroke to adhere to an intensive treatment target (systolic blood pressure, <120 mm Hg) or a standard treatment target (systolic blood pressure, <140 mm Hg). The primary outcome was a composite of myocardial infarction, other acute coronary syndromes, stroke, acute decompensated heart failure, or death from cardiovascular causes. Additional primary outcome events occurring through the end of the intervention period (August 20, 2015) were adjudicated after data lock for the primary analysis. We also analyzed post-trial observational follow-up data through July 29, 2016.
Results: At a median of 3.33 years of follow-up, the rate of the primary outcome and all-cause mortality during the trial were significantly lower in the intensive-treatment group than in the standard-treatment group (rate of the primary outcome, 1.77% per year vs. 2.40% per year; hazard ratio, 0.73; 95% confidence interval [CI], 0.63 to 0.86; all-cause mortality, 1.06% per year vs. 1.41% per year; hazard ratio, 0.75; 95% CI, 0.61 to 0.92). Serious adverse events of hypotension, electrolyte abnormalities, acute kidney injury or failure, and syncope were significantly more frequent in the intensive-treatment group. When trial and post-trial follow-up data were combined (3.88 years in total), similar patterns were found for treatment benefit and adverse events; however, rates of heart failure no longer differed between the groups.
Conclusions: Among patients who were at increased cardiovascular risk, targeting a systolic blood pressure of less than 120 mm Hg resulted in lower rates of major adverse cardiovascular events and lower all-cause mortality than targeting a systolic blood pressure of less than 140 mm Hg, both during receipt of the randomly assigned therapy and after the trial. Rates of some adverse events were higher in the intensive-treatment group. (Funded by the National Institutes of Health; SPRINT ClinicalTrials.gov number, NCT01206062.).
Copyright © 2021 Massachusetts Medical Society.
Figures
Comment in
-
A SPRINT towards tighter control of blood pressure in hypertension.Eur Heart J. 2021 Aug 21;42(32):3042-3043. doi: 10.1093/eurheartj/ehab400. Eur Heart J. 2021. PMID: 34173000 No abstract available.
-
Are blood-pressure targets needed to prevent cardiovascular disease?Nat Rev Cardiol. 2021 Sep;18(9):615-616. doi: 10.1038/s41569-021-00595-4. Nat Rev Cardiol. 2021. PMID: 34230648 No abstract available.
References
-
- Systolic Blood Pressure Intervention Trial (SPRINT) protocol version 4.0. November 1, 2012. (https://www.sprinttrial.org/public/Protocol_Current.pdf).
-
- Correction to: A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2017;3 77: 2506. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UL1 TR000433/TR/NCATS NIH HHS/United States
- UL1 TR000445/TR/NCATS NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- UL1 TR002538/TR/NCATS NIH HHS/United States
- UL1 TR000093/TR/NCATS NIH HHS/United States
- P30 AG049638/AG/NIA NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000050/TR/NCATS NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- U54 TR000123/TR/NCATS NIH HHS/United States
- HHSN268200900048C/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- HHSN268200900040C/HL/NHLBI NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- HHSN268200900046C/HL/NHLBI NIH HHS/United States
- P30 GM103337/GM/NIGMS NIH HHS/United States
- UL1 TR001064/TR/NCATS NIH HHS/United States
- UL1 RR025752/RR/NCRR NIH HHS/United States
- UL1 RR025771/RR/NCRR NIH HHS/United States
- HHSN268200900049C/HL/NHLBI NIH HHS/United States
- HHSN268200900047C/HL/NHLBI NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000073/TR/NCATS NIH HHS/United States
- UL1 TR000002/TR/NCATS NIH HHS/United States
- UL1 TR000105/TR/NCATS NIH HHS/United States
- UL1 RR024134/RR/NCRR NIH HHS/United States
- UL1 TR003142/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical