

Antibody-mediated procoagulant platelets in SARS-CoV-2-vaccination associated immune thrombotic thrombocytopenia
- PMID: 34011137
- PMCID: PMC8327736
- DOI: 10.3324/haematol.2021.279000
Antibody-mediated procoagulant platelets in SARS-CoV-2-vaccination associated immune thrombotic thrombocytopenia
Abstract
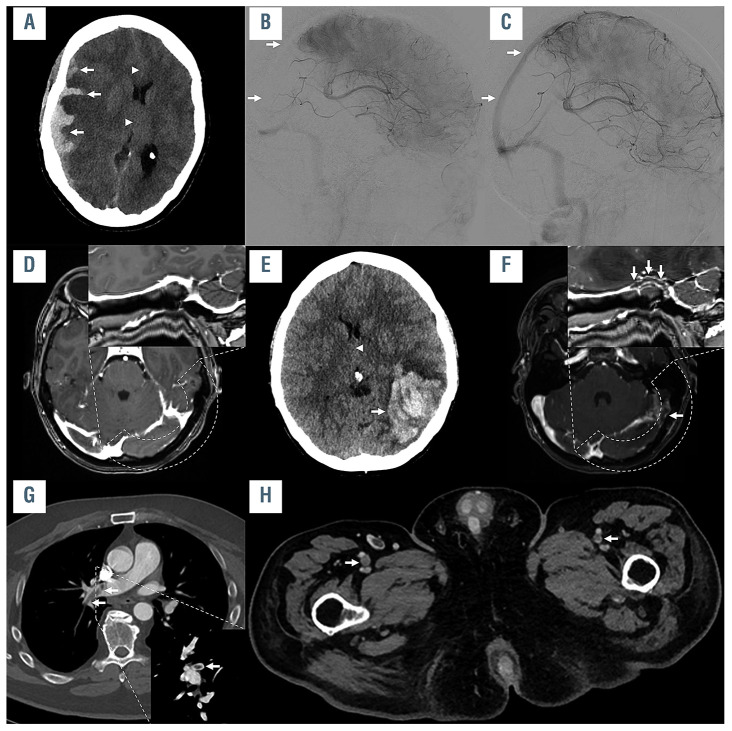
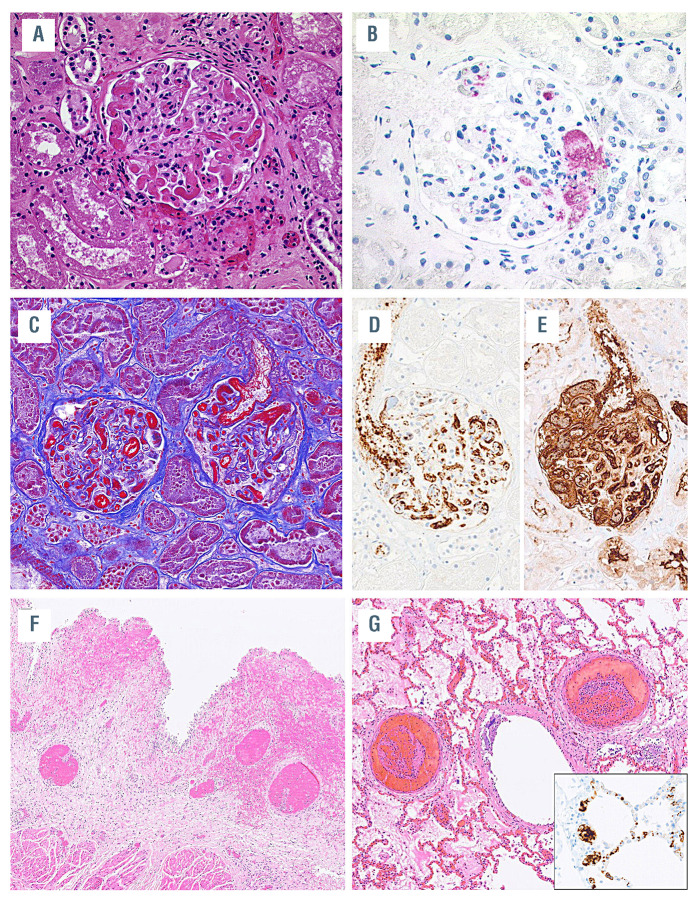
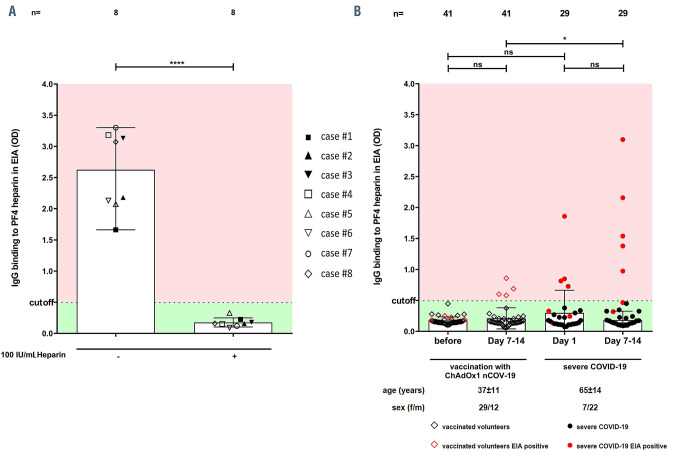
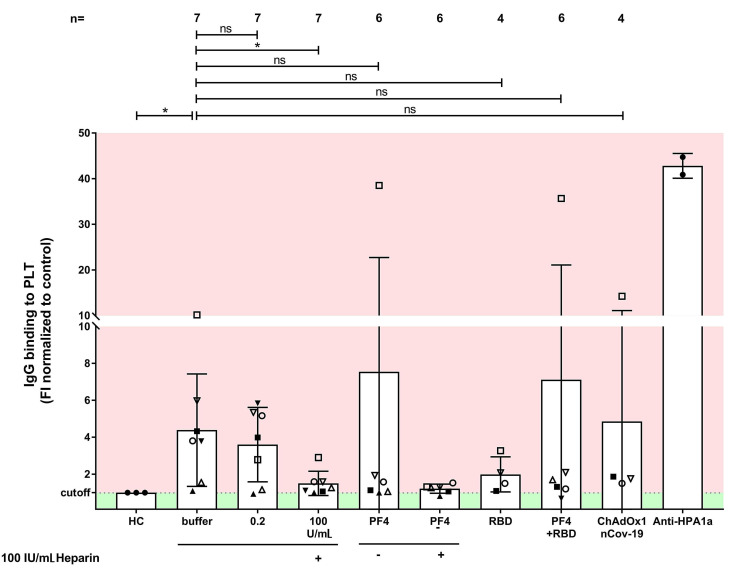
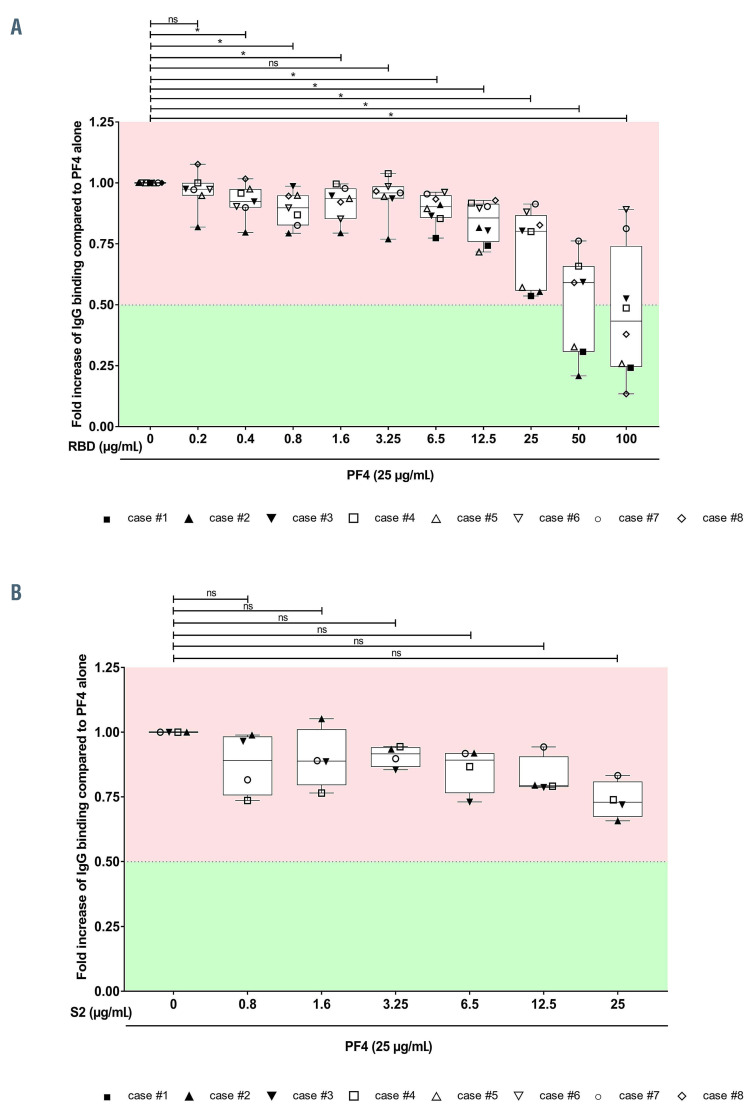
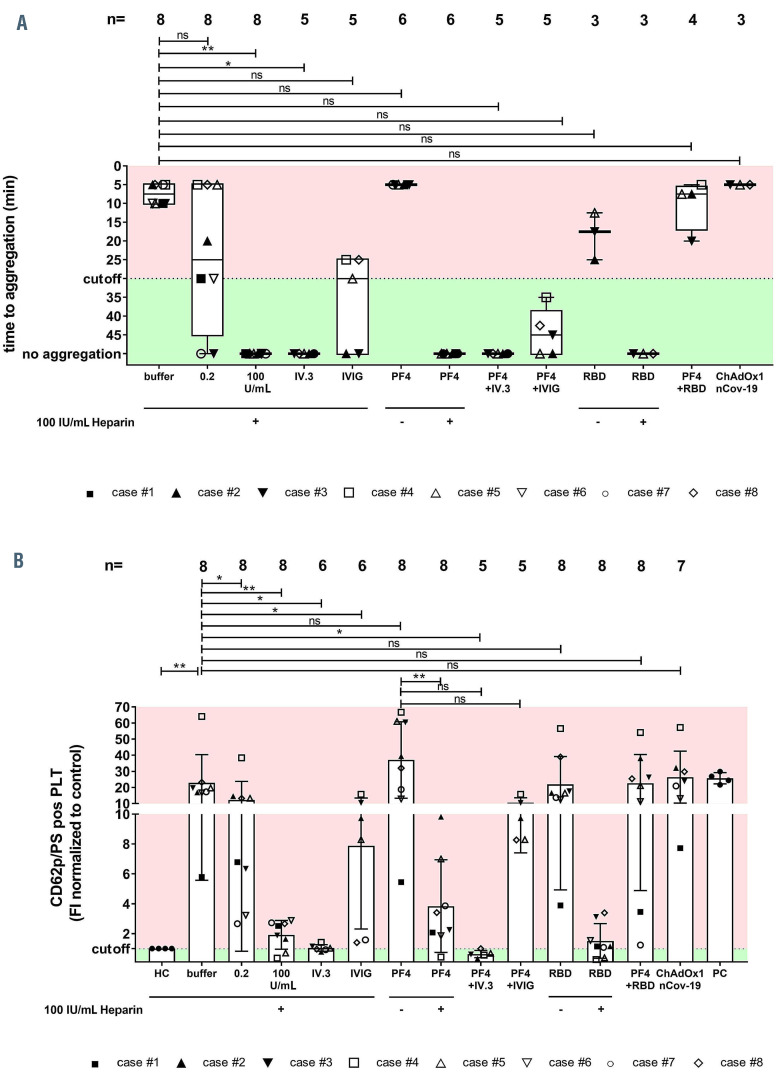
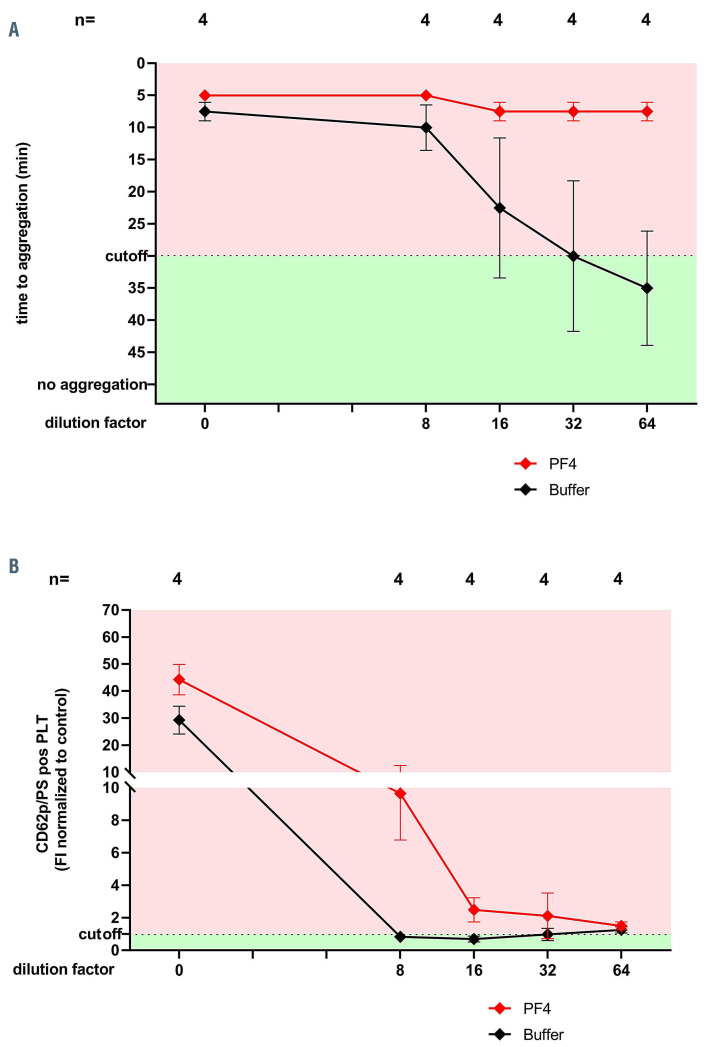
The COVID-19 pandemic has resulted in significant morbidity and mortality worldwide. To prevent severe infection, mass COVID-19 vaccination campaigns with several vaccine types are currently underway. We report pathological and immunological findings in 8 patients who developed vaccine-induced immune thrombotic thrombocytopenia (VITT) after administration of SARS-CoV-2 vaccine ChAdOx1 nCoV-19. We analyzed patient material using enzyme immune assays, flow cytometry and heparin-induced platelet aggregation assay and performed autopsies on two fatal cases. Eight patients (5 female, 3 male) with a median age of 41.5 years (range, 24 to 53) were referred to us with suspected thrombotic complications 6 to 20 days after ChAdOx1 nCoV-19 vaccination. All patients had thrombocytopenia at admission. Patients had a median platelet count of 46.5 x109/L (range, 8 to 92). Three had a fatal outcome and 5 were successfully treated. Autopsies showed arterial and venous thromboses in various organs and the occlusion of glomerular capillaries by hyaline thrombi. Sera from VITT patients contain high titer antibodies against platelet factor 4 (PF4) (OD 2.59±0.64). PF4 antibodies in VITT patients induced significant increase in procoagulant markers (P-selectin and phosphatidylserine externalization) compared to healthy volunteers and healthy vaccinated volunteers. The generation of procoagulant platelets was PF4 and heparin dependent. We demonstrate the contribution of antibody-mediated platelet activation in the pathogenesis of VITT.
Figures
Comment in
-
A new enemy is emerging in the fight against the SARS-CoV-2 pandemic.Haematologica. 2021 Aug 1;106(8):2040-2041. doi: 10.3324/haematol.2021.279186. Haematologica. 2021. PMID: 34011139 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
