

Guy's and St Thomas NHS Foundation active surveillance prostate cancer cohort: a characterisation of a prostate cancer active surveillance database
- PMID: 34011308
- PMCID: PMC8135162
- DOI: 10.1186/s12885-021-08255-z
Guy's and St Thomas NHS Foundation active surveillance prostate cancer cohort: a characterisation of a prostate cancer active surveillance database
Erratum in
-
Correction to: Guy's and St Thomas NHS Foundation active surveillance prostate cancer cohort: a characterisation of a prostate cancer active surveillance database.BMC Cancer. 2022 Jan 24;22(1):97. doi: 10.1186/s12885-022-09188-x. BMC Cancer. 2022. PMID: 35073850 Free PMC article. No abstract available.
Abstract
Background: The routine clinical use of serum prostatic specific antigen (PSA) testing has allowed earlier detection of low-grade prostate cancer (PCa) with more favourable characteristics, leading to increased acceptance of management by active surveillance (AS). AS aims to avoid over treatment in men with low and intermediate-risk PCa and multiple governing bodies have described several AS protocols. This study provides a descriptive profile of the Guy's and St Thomas NHS Foundation Trust (GSTT) AS cohort as a platform for future research in AS pathways in PCa.
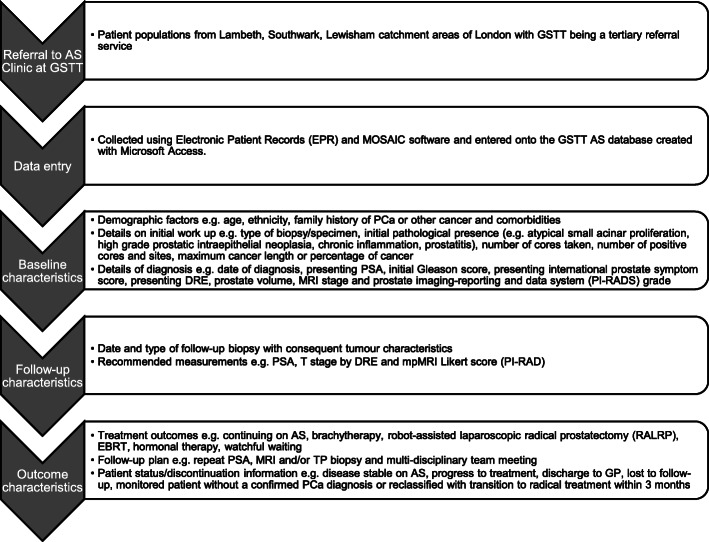
Methods: Demographic and baseline characteristics were retrospectively collected in a database for patients at the GSTT AS clinic with prospective collection of follow-up data from 2012. Seven hundred eighty-eight men being monitored at GSTT with histologically confirmed intermediate-risk PCa, at least 1 follow-up appointment and diagnostic characteristics consistent with AS criteria were included in the profile. Descriptive statistics, Kaplan-Meier survival curves and multivariable Cox proportion hazards regression models were used to characterize the cohort.
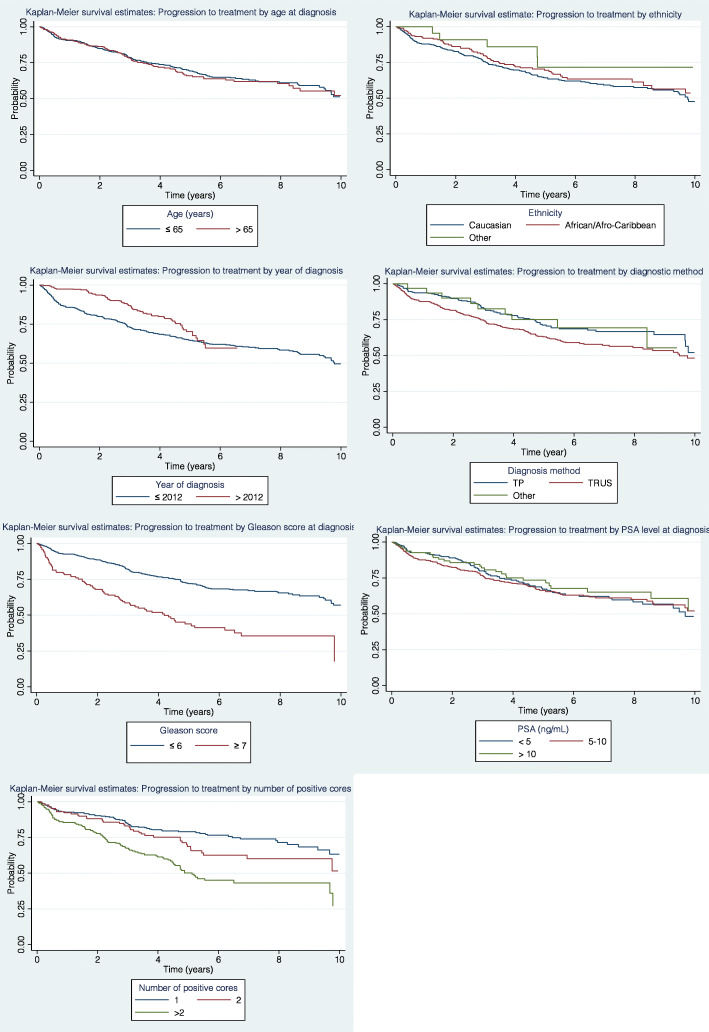
Discussion: A relatively large proportion of the cohort includes men of African/Afro-Caribbean descent (22%). More frequent use of magnetic resonance imaging and trans-perineal biopsies at diagnosis was observed among patients diagnosed after 2012. Those who underwent trans-rectal ultrasound diagnostic biopsy received their first surveillance biopsy 20 months earlier than those who underwent trans-perineal diagnostic biopsy. At 3 years, 76.1% men remained treatment free. Predictors of treatment progression included Gleason score 3 + 4 (Hazard ratio (HR): 2.41, 95% Confidence interval (CI): 1.79-3.26) and more than 2 positive cores taken at biopsy (HR: 2.65, CI: 1.94-3.62). A decreased risk of progressing to treatment was seen among men diagnosed after 2012 (HR: 0.72, CI: 0.53-0.98).
Conclusion: An organised biopsy surveillance approach, via two different AS pathways according to the patient's diagnostic method, can be seen within the GSTT cohort. Risk of patients progressing to treatment has decreased in the period since 2012 compared with the prior period with more than half of the cohort remaining treatment free at 5 years, highlighting that the fundamental aims of AS at GSTT are being met. Thus, this cohort is a good resource to investigate the AS treatment pathway.
Keywords: Active surveillance; Cohort; Prostate cancer.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures

References
-
- Mazzucchelli R, Nesseris I, Cheng L, Lopez-Beltran A, Montironi R, Scarpelli M. Active surveillance for low-risk prostate cancer. Anticancer Res. 2010;30(9):3683–92. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
