

Electronic clinical decision support for children with minor head trauma and intracranial injuries: a sociotechnical analysis
- PMID: 34011315
- PMCID: PMC8132484
- DOI: 10.1186/s12911-021-01522-w
Electronic clinical decision support for children with minor head trauma and intracranial injuries: a sociotechnical analysis
Abstract
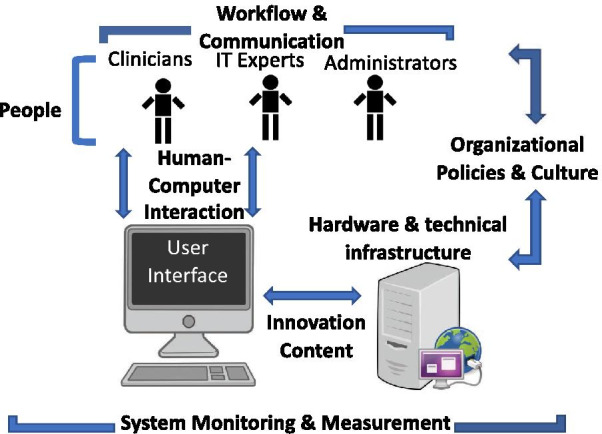
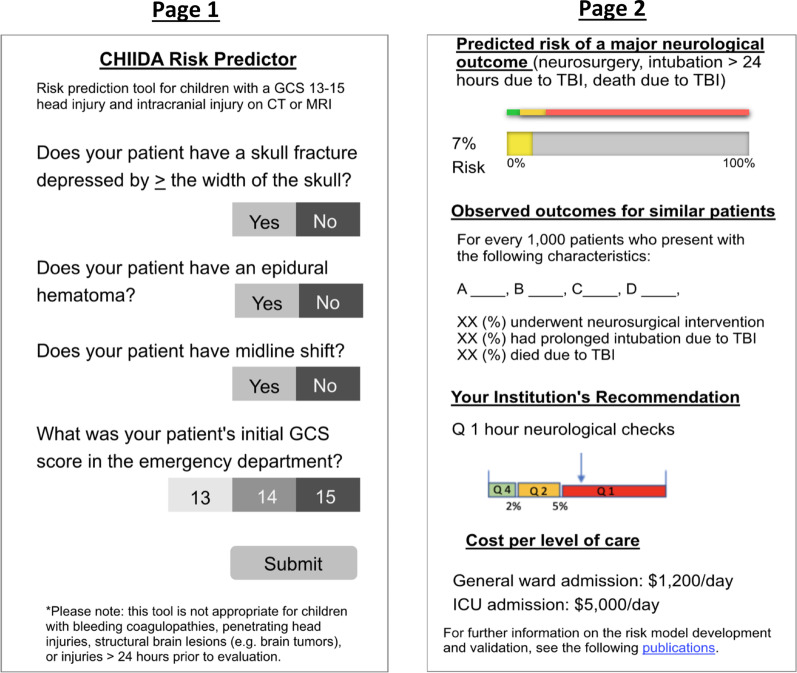
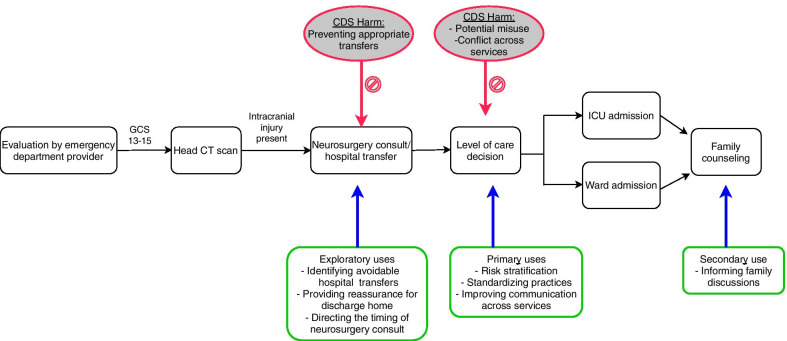
Background: Current management of children with minor head trauma (MHT) and intracranial injuries is not evidence-based and may place some children at risk of harm. Evidence-based electronic clinical decision support (CDS) for management of these children may improve patient safety and decrease resource use. To guide these efforts, we evaluated the sociotechnical environment impacting the implementation of electronic CDS, including workflow and communication, institutional culture, and hardware and software infrastructure, among other factors.
Methods: Between March and May, 2020 semi-structured qualitative focus group interviews were conducted to identify sociotechnical influences on CDS implementation. Physicians from neurosurgery, emergency medicine, critical care, and pediatric general surgery were included, along with information technology specialists. Participants were recruited from nine health centers in the United States. Focus group transcripts were coded and analyzed using thematic analysis. The final themes were then cross-referenced with previously defined sociotechnical dimensions.
Results: We included 28 physicians and four information technology specialists in seven focus groups (median five participants per group). Five physicians were trainees and 10 had administrative leadership positions. Through inductive thematic analysis, we identified five primary themes: (1) clinical impact; (2) stakeholders and users; (3) tool content; (4) clinical practice integration; and (5) post-implementation evaluation measures. Participants generally supported using CDS to determine an appropriate level-of-care for these children. However, some had mixed feelings regarding how the tool could best be used by different specialties (e.g. use by neurosurgeons versus non-neurosurgeons). Feedback from the interviews helped refine the tool content and also highlighted potential technical and workflow barriers to address prior to implementation.
Conclusions: We identified key factors impacting the implementation of electronic CDS for children with MHT and intracranial injuries. These results have informed our implementation strategy and may also serve as a template for future efforts to implement health information technology in a multidisciplinary, emergency setting.
Keywords: Electronic clinical decision support; Head trauma; Health information technology; Implementation science; Sociotechnical analysis; Traumatic brain injury.
Conflict of interest statement
Dr. Randi Foraker is a member of the editorial board of BMC Medical Informatics and Decision Making.
Figures
References
-
- National Center for Injury Prevention and Control. Report to Congress on Mild Traumatic Brain Injury in the United States: Steps to Prevent a Serious Public Health Problem. Atlanta, GA 2003.
-
- Lumba-Brown A, Yeates KO, Sarmiento K, Breiding MJ, Haegerich TM, Gioia GA, et al. Centers for disease control and prevention guideline on the diagnosis and management of mild traumatic brain injury among children. JAMA Pediatr. 2018;172(11):e182853. doi: 10.1001/jamapediatrics.2018.2853. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
