

Postnatal steroid management in preterm infants with evolving bronchopulmonary dysplasia
- PMID: 34012057
- PMCID: PMC8133053
- DOI: 10.1038/s41372-021-01083-w
Postnatal steroid management in preterm infants with evolving bronchopulmonary dysplasia
Abstract
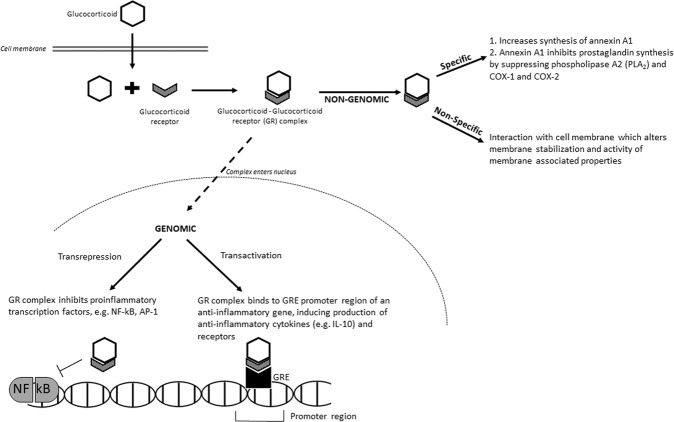
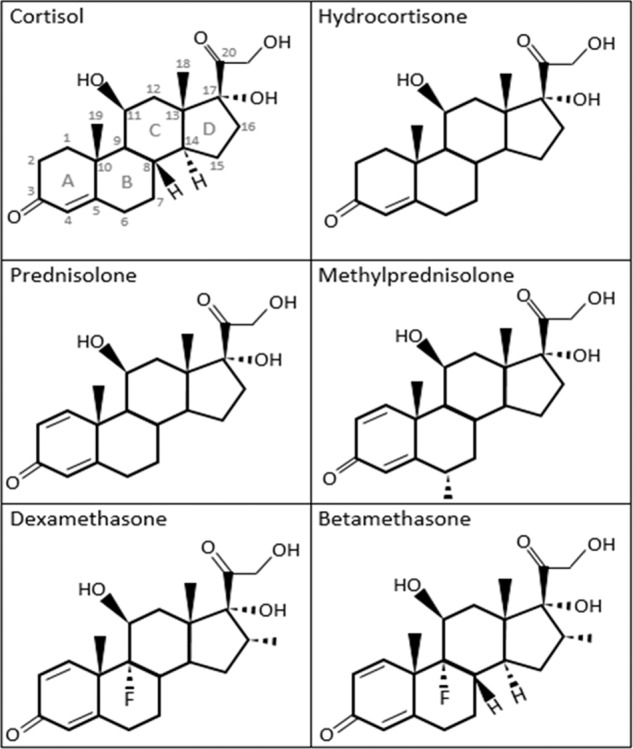
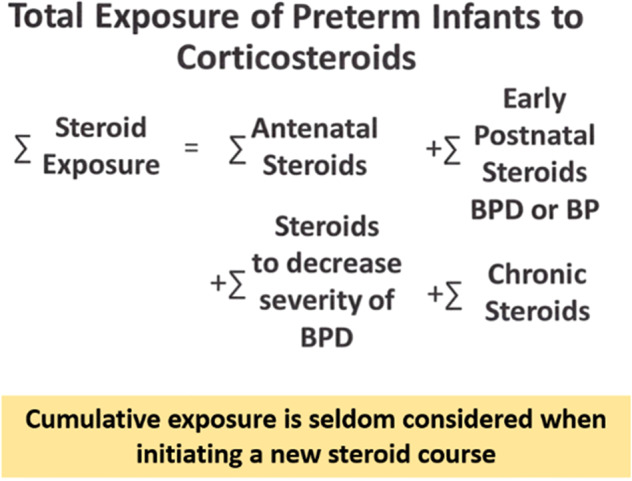
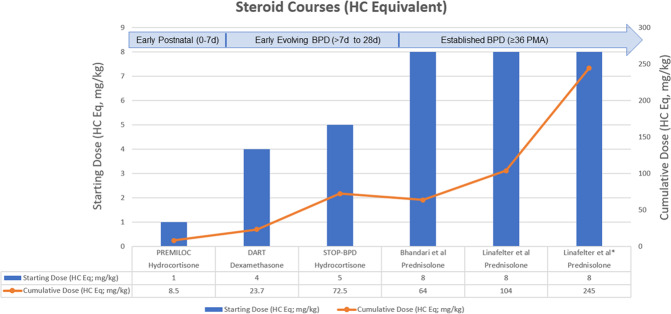
Bronchopulmonary dysplasia (BPD) is a chronic lung disease commonly affecting extremely preterm infants. Although mechanical ventilation and oxygen requirements in premature infants are identified as inciting mechanisms for inflammation and the development of BPD over time, data now support an array of perinatal events that may stimulate the inflammatory cascade prior to delivery. Corticosteroids, such as dexamethasone and hydrocortisone, have proven beneficial for the prevention and management of BPD postnatally due to their anti-inflammatory characteristics. This review aims to examine the pharmacologic properties of several corticosteroids, appraise the existing evidence for postnatal corticosteroid use in preterm infants, and assess steroid management strategies to ameliorate BPD. Finally, we aim to provide guidance based on clinical experience for managing adrenal suppression resulting from prolonged steroid exposure since this is an area less well-studied.
© 2021. This is a U.S. government work and not under copyright protection in the U.S.; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
