

A Novel Non-Invasive Device for the Assessment of Central Venous Pressure in Hospital, Office and Home
- PMID: 34012302
- PMCID: PMC8128499
- DOI: 10.2147/MDER.S307775
A Novel Non-Invasive Device for the Assessment of Central Venous Pressure in Hospital, Office and Home
Abstract
Background: Venous congestion can be quantified by central venous pressure (CVP) and its monitoring is crucial to understand and follow the hemodynamic status of patients with cardio-respiratory diseases. The standard technique for CVP measurement is invasive, requiring the insertion of a catheter into a jugular vein, with potential complications. On the other hand, the current non-invasive methods, mainly based on ultrasounds, remain operator-dependent and are unsuitable for use in the home environment. In this paper, we will introduce a novel, non-invasive device for the hospital, office and home assessment of CVP.
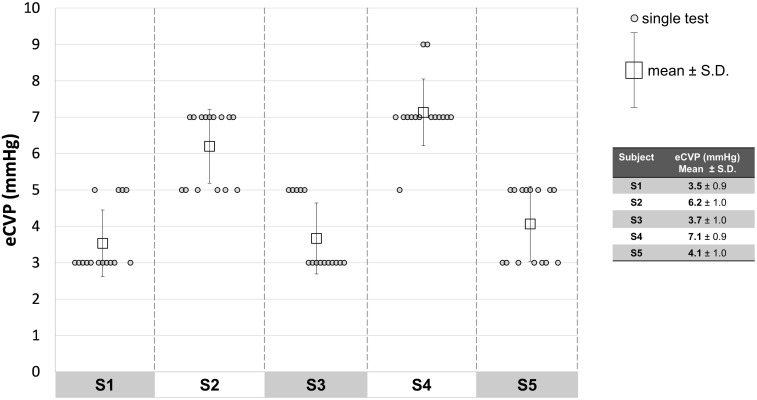
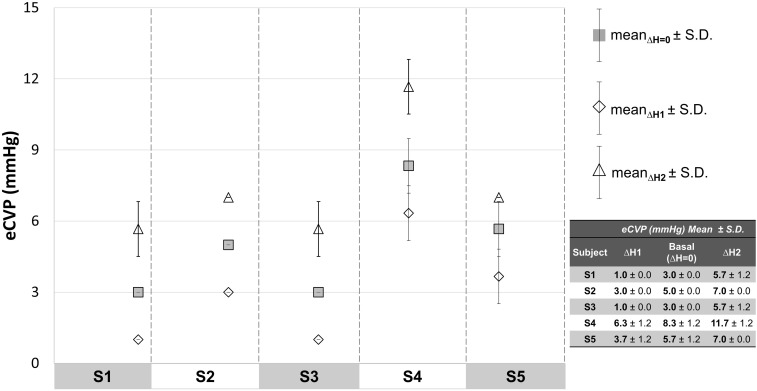
Methods: After describing the measurement concept, we will report a preliminary experimental study enrolling 5 voluntary healthy subjects to evaluate the VenCoM measurements' repeatability, and the system's capability in measuring small elicited venous pressure variations (2 mmHg), as well as an induced venous hypertension within a pathological range (12÷20 mmHg).
Results: The experimental measurements showed a repeatability of ±1mmHg. The VenCoM device was able to reliably detect the elicited venous pressure variations and the simulated congestive status.
Discussion and conclusion: The proposed non-invasive VenCoM device is able to provide a fast and repeatable CVP estimate, having a wide spectrum of potential clinical applications, including the monitoring of venous congestion in heart failure patients and in subjects with renal and hepatic dysfunction, as well as pulmonary hypertension (PH) that can be extended to pneumonia COVID-19 patients even after recovery. The device needs to be tested further on a large sample size of both healthy and pathological subjects, to systematically validate its reliability and impact in clinical setting.
Keywords: COVID-19; cardiovascular measurements; central venous pressure; heart failure; home monitoring; non-invasive device; pulmonary artery pressure.
© 2021 Marcelli et al.
Conflict of interest statement
E.M., L.C., B.B. have served as consultants for TRE ESSE Progettazione Biomedica srl. within the consultancy agreement between DIMES Department of Alma Mater Studiorum - Università di Bologna, and TRE ESSE Progettazione Biomedica srl. G.P. is the Scientific Director of TRE ESSE Progettazione Biomedica srl; in addition, G.P. has patents pending: 1 Italian Patent Application (IT201900010248, Filed: 27 June 2019); Dispositivo per la rilevazione della pressione venosa; Applicant: TRE ESSE Progettazione Biomedica srl; Inventor: Gianni Plicchi; 1 PCT Application (PCT/IB2020/055060, Filed 28 May 2020): Device for venous pressure sensing; Applicant: TRE ESSE Progettazione Biomedica srl; Inventor: Gianni Plicchi. The authors reported no other potential conflicts of interest for this work.
Figures










References
LinkOut - more resources
Full Text Sources
Other Literature Sources
