

Transbronchial microwave ablation of lung nodules with electromagnetic navigation bronchoscopy guidance-a novel technique and initial experience with 30 cases
- PMID: 34012778
- PMCID: PMC8107744
- DOI: 10.21037/tlcr-20-1231
Transbronchial microwave ablation of lung nodules with electromagnetic navigation bronchoscopy guidance-a novel technique and initial experience with 30 cases
Abstract
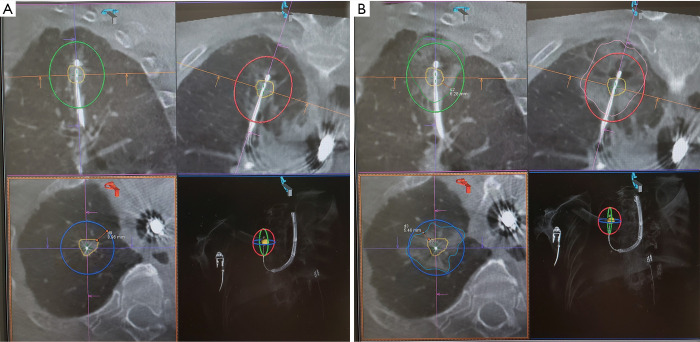
Background: Microwave ablation of lung nodules may provide a faster, larger and more predictable ablation zone than other energy sources, while bronchoscopic transbronchial ablation has theoretical advantage of fewer pleural-based complications than percutaneous approach. Our study aims to determine whether the novel combination of bronchoscopic approach and microwave ablation in management of lung nodules is technically feasible, safe and effective.
Methods: This is a retrospective analysis of a single center experience in electromagnetic navigation bronchoscopy microwave ablation in hybrid operating room. Patients had high surgical risks while lung nodules were either proven malignant or radiologically suspicious. Primary endpoints include technical feasibility and safety.
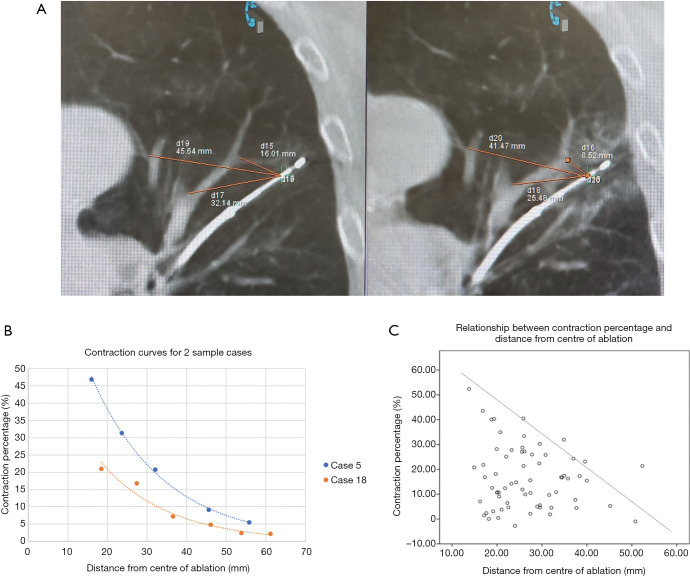
Results: Total of 30 lung nodules from 25 patients were treated. Mean nodule size was 15.1 mm, and bronchus directly leads to the nodules (bronchus sign positive) in only half of them. Technical success rate was 100%, although some nodules required double ablation for adequate coverage. Mean minimal ablation margin was 5.51 mm. The mean actual ablation zone volume was -21.4% compared to predicted, likely due to significant tissue contraction ranging from 0-43%. There was no significant heat sink effect. Mean hospital stay was 1.73 days, and only 1 patient stayed for more than 3 days. Complications included pain (13.3%), pneumothorax requiring drainage (6.67%), post-ablation reaction (6.67%), pleural effusion (3.33%) and hemoptysis (3.33%). After median follow up of 12 months, none of the nodules had evidence of progression.
Conclusions: Bronchoscopic transbronchial microwave ablation is safe and feasible for treatment of malignant lung nodules. Prospective study on clinical application of this novel technique is warranted.
Keywords: Microwave ablation; electromagnetic navigation bronchoscopy; hybrid operating room; lung cancer; transbronchial ablation.
2021 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at Available at http://dx.doi.org/10.21037/tlcr-20-1231). CSHN is a consultant for Johnson and Johnson; Medtronic, USA; and Siemens Healthineer. RWHL is a consultant for Medtronic, USA; and Siemens Healthineer. TSKM has no potential conflicts of interest that exist with companies/organizations whose products or services are discussed in this article. The other authors have no conflicts of interest to declare.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources