

Plasma pre-treatment T790M relative allelic frequency in patients with advanced EGFR-mutated non-small cell lung cancer predicts treatment response to subsequent-line osimertinib
- PMID: 34012779
- PMCID: PMC8107763
- DOI: 10.21037/tlcr-20-1125
Plasma pre-treatment T790M relative allelic frequency in patients with advanced EGFR-mutated non-small cell lung cancer predicts treatment response to subsequent-line osimertinib
Abstract
Background: Approximately half of all patients with advanced EGFR-mutant NSCLC will develop acquired resistance to first or second-generation EGFR tyrosine kinase inhibitors (EGFR-TKIs) with a T790M mutation. In the AURA3 trial, patients with a T790M mutation had a response rate of 71% to osimertinib, a third-generation EGFR-TKI. The response to osimertinib may vary according to plasma T790M mutation frequency. Our aim was to determine the effect of plasma T790M mutation load on treatment response to osimertinib in an Australian multi-institutional cohort.
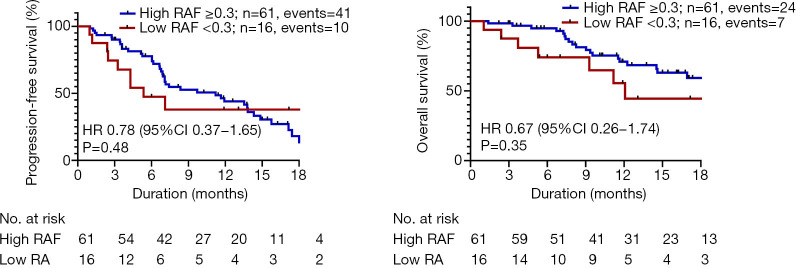
Methods: We performed a retrospective study on patients treated with osimertinib in the second-line setting and beyond between 2016-2018 from ten centres in Australia, who had T790M mutations detected in tumour or plasma. The primary objective was to investigate if there was a difference in disease control rate (DCR) between patients with high vs. low T790M relative allelic frequency (RAF) as detected in plasma, using a 0.3 RAF cut-off, as determined by ddPCR or BEAMing PCR. Secondary objective was to determine the survival outcomes according to high versus low plasma T790M RAF. Additional analyses were performed to investigate the survival outcome for patients with plasma versus tissue T790M positivity.
Results: A total of 139 patients were included in this study. Patients with higher RAF demonstrated higher DCR (74% vs. 36%, P=0.02), however there was no statistically significant difference in survival outcomes in the two groups. Exploratory analysis showed that patients with tissue T790M+ had improved DCR compared with those with plasma T790M+ (89% vs. 68%, P=0.01) and longer progression free survival (median 15.4 vs. 9.7 months; HR 0.51, 95% CI: 0.34 to 0.77, P=0.003) and overall survival (median not reached, HR 0.51, 95% CI: 0.30 to 0.86, P=0.02). Patients who were tissue T790M+ demonstrated superior survival compared to plasma T790M+ after correcting for confounding variables in a multivariate model.
Conclusions: DCR was superior in patients with higher plasma T790M mutation load versus lower plasma T790M mutational load, without significant survival benefit. Plasma T790M RAF is a potential predictive biomarker which should be investigated and validated in larger prospective studies.
Keywords: Circulating tumour DNA; T790M relative allelic frequency; epidermal growth factor receptor; liquid biopsy; non-small cell lung cancer (NSCLC).
2021 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/tlcr-20-1125). Dr. Ding reports grants from Astrazeneca, during the conduct of the study; personal fees from Roche, personal fees from Astrazeneca, outside the submitted work; Dr. Lee reports grants and personal fees from Astrazeneca, personal fees from Boehringer Ingelheim, personal fees from Norvatis, personal fees from Pfizer, personal fees from Roche, outside the submitted work; Dr. Itchins reports personal fees from Astrazeneca, personal fees from Roche, personal fees from MSD, personal fees from Pfizer, personal fees from Takeda, personal fees from Novartis, outside the submitted work; Dr. Clarke reports personal fees from Astrazeneca, outside the submitted work; Dr. Blinman reports personal fees from Astrazeneca, personal fees from Boehringer Ingelheim, outside the submitted work; Dr. Kao reports personal fees from Astrazeneca, personal fees from Boehringer Ingelheim, personal fees from Pfizer, personal fees from MSD, personal fees from BMS, personal fees from Takeda, personal fees from Roche, outside the submitted work; Dr. John reports personal fees from Roche, personal fees from BMS, personal fees from Merck, personal fees from Ignyta, personal fees from Astrazeneca, personal fees from Takeda, personal fees from MSD, personal fees from Specialised therapeutics, personal fees from Pfizer, outside the submitted work; Dr. Leal reports grants and personal fees from Roche, grants and personal fees from BMS, grants and personal fees from Astrazeneca, grants and personal fees from MSD, grants and personal fees from Pfizer, grants and personal fees from Boehringher Ingelheim, personal fees from Sanofi, personal fees from Elly-Lilly, personal fees from Tecnofarma, outside the submitted work. The other authors have no conflicts of interest to declare.
Figures



References
-
- Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol 2010;11:121-8. 10.1016/S1470-2045(09)70364-X - DOI - PubMed
-
- Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol 2012;13:239-46. 10.1016/S1470-2045(11)70393-X - DOI - PubMed
-
- Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol 2011;12:735-42. 10.1016/S1470-2045(11)70184-X - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous