

Hyperkalemia and its Association With Mortality, Cardiovascular Events, Hospitalizations, and Intensive Care Unit Admissions in a Population-Based Retrospective Cohort
- PMID: 34013109
- PMCID: PMC8116905
- DOI: 10.1016/j.ekir.2021.02.038
Hyperkalemia and its Association With Mortality, Cardiovascular Events, Hospitalizations, and Intensive Care Unit Admissions in a Population-Based Retrospective Cohort
Abstract
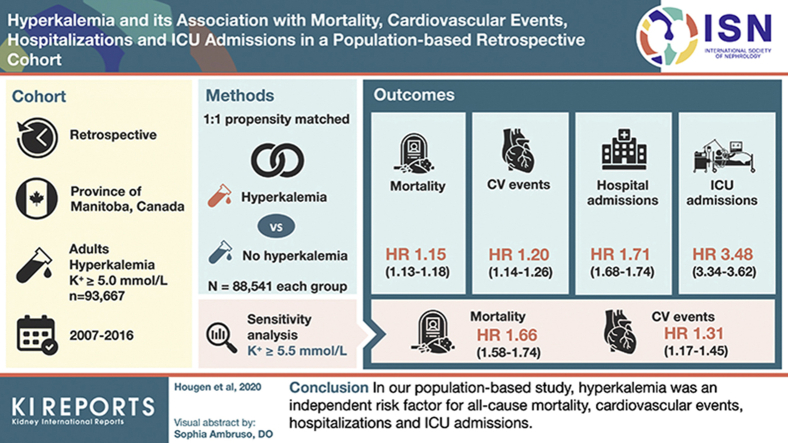
Introduction: Hyperkalemia is a common, potentially life-threatening condition in patients with chronic kidney disease (CKD). We studied the association between hyperkalemia and mortality, cardiovascular events, hospitalizations, and intensive care unit (ICU) admissions.
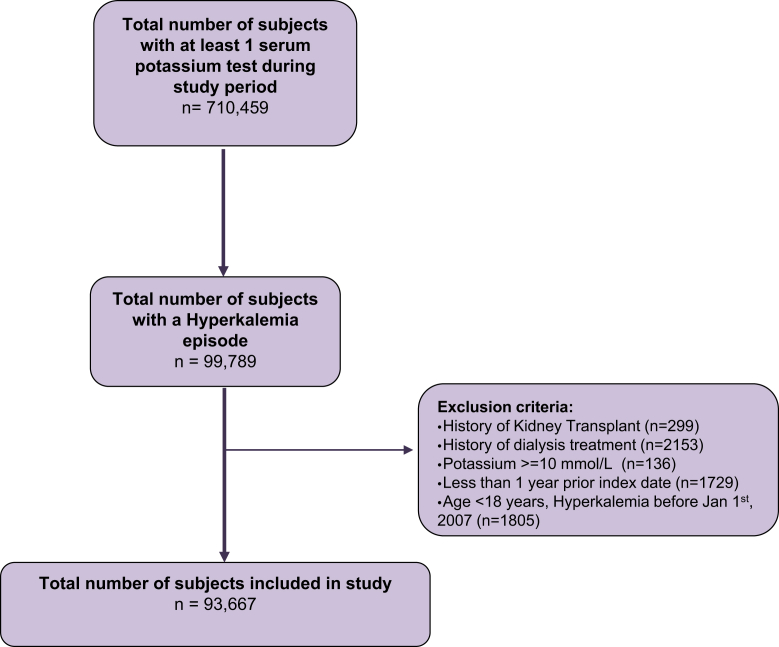
Methods: We performed a retrospective cohort study using administrative databases in Manitoba, Canada. All adults (≥18 years of age) with potassium tests between January 2007 and December 2016 were included, with follow-up until March 31, 2017. Propensity score matching was performed among patients with de novo hyperkalemia (serum potassium ≥ 5.0 mmol/l) and patients who were nonhyperkalemic. The association between hyperkalemia and normokalemia and mortality was assessed using multivariate Cox proportional hazards regression models, adjusting for patient characteristics in a 1:1 propensity score-matched sample. Secondary outcomes included cardiovascular events, hospitalizations, and ICU admissions. A sensitivity analysis was performed with hyperkalemia defined as serum potassium ≥ 5.5 mmol/l.
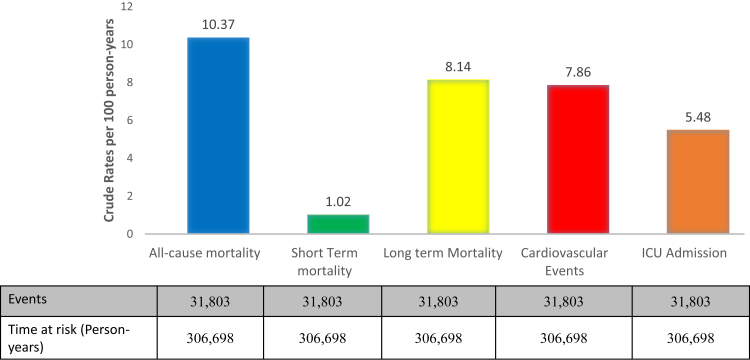
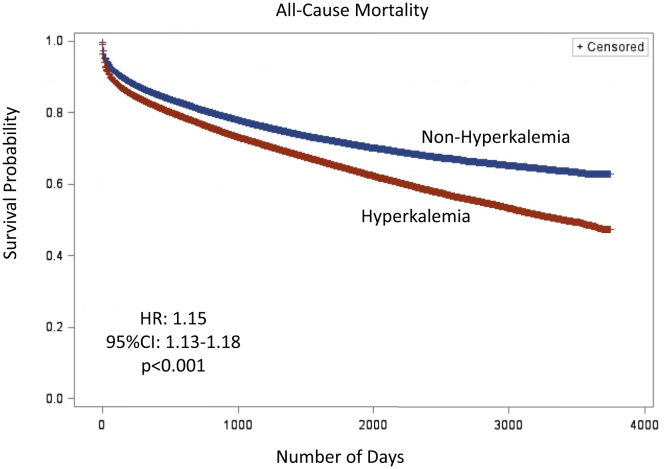
Results: Of 93,667 patients with de novo hyperkalemia, 36% had diabetes mellitus (DM), 28% had CKD, and 21% had heart failure (HF). In the propensity score-matched sample of 177,082 individuals, hyperkalemia was associated with an increased risk for all-cause mortality (hazard ratio [HR] 1.15 [95% confidence interval {CI} 1.13-1.18], P < 0.001), cardiovascular events (HR 1.20 [95% CI 1.14-1.26], P < 0.001), short-term mortality (odds ratio [OR] 1.29 [95% CI 1.24-1.34], P < 0.001), hospitalizations (OR 1.71 [95% CI 1.68-1.74]), and ICU admissions (OR 3.48 [95% CI 3.34-3.62], P < 0.001). Findings were unchanged when a threshold of serum potassium ≥ 5.5 mmol/l was used.
Conclusion: Hyperkalemia was an independent risk factor for all-cause mortality, cardiovascular events, hospitalizations, and ICU admissions. This finding expands our understanding of important clinical outcomes associated with hyperkalemia.
Keywords: diabetes; hyperkalemia; kidney disease; mortality; population.
© 2021 International Society of Nephrology. Published by Elsevier Inc.
Figures
Comment in
-
Is It Time to Rethink the Age-Old Practice of Permissive Hyperkalemia in Renin-Angiotensin-Aldosterone Inhibition?Kidney Int Rep. 2021 Apr 3;6(5):1203-1204. doi: 10.1016/j.ekir.2021.03.895. eCollection 2021 May. Kidney Int Rep. 2021. PMID: 34015068 Free PMC article. No abstract available.
References
-
- Gilligan S., Raphael K. Hyperkalemia and hypokalemia in CKD: prevalence, risk factors, and clinical outcomes. Adv Chronic Kidney Dis. 2017;24:315–318. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
