

This is a preprint.
Impaired immune signaling and changes in the lung microbiome precede secondary bacterial pneumonia in COVID-19
- PMID: 34013247
- PMCID: PMC8132240
- DOI: 10.21203/rs.3.rs-380803/v1
Impaired immune signaling and changes in the lung microbiome precede secondary bacterial pneumonia in COVID-19
Abstract
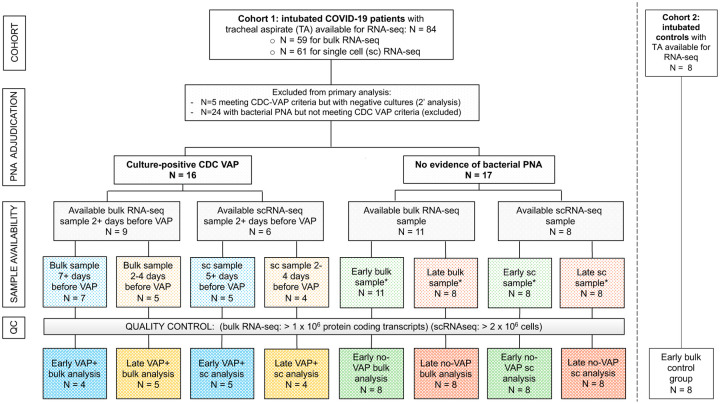
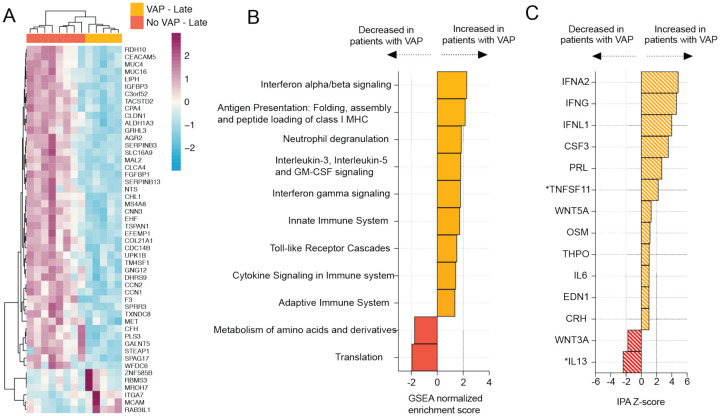
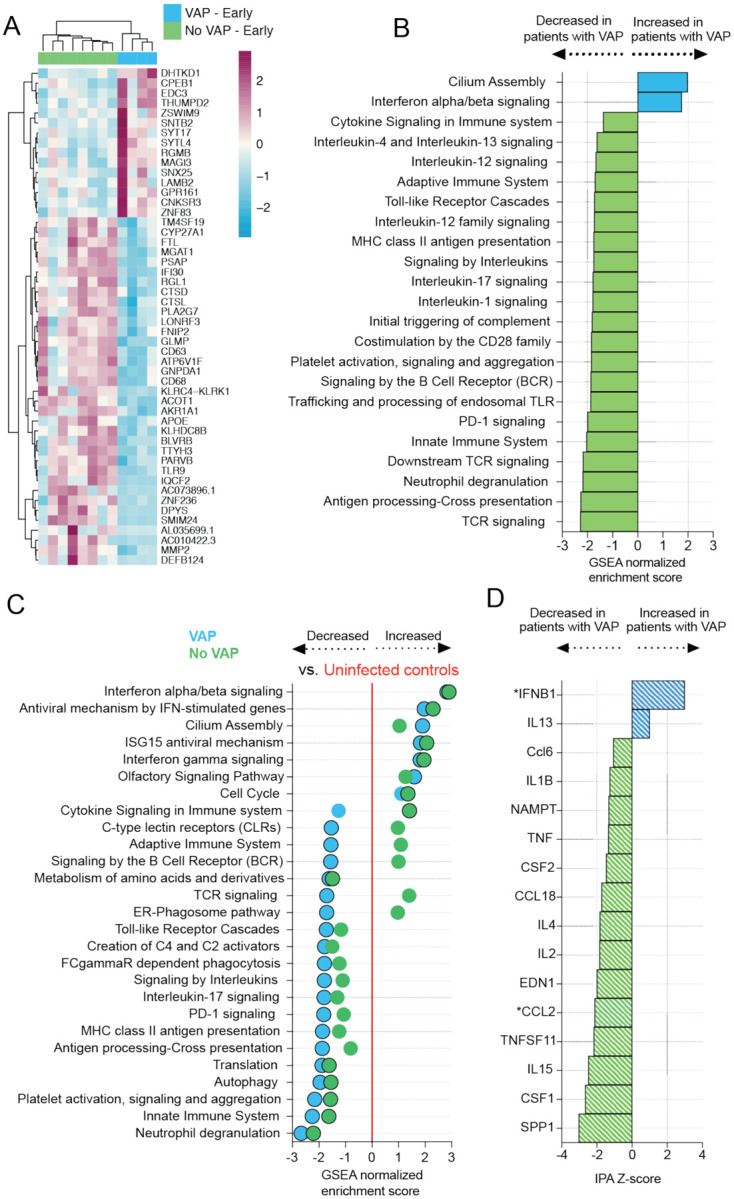
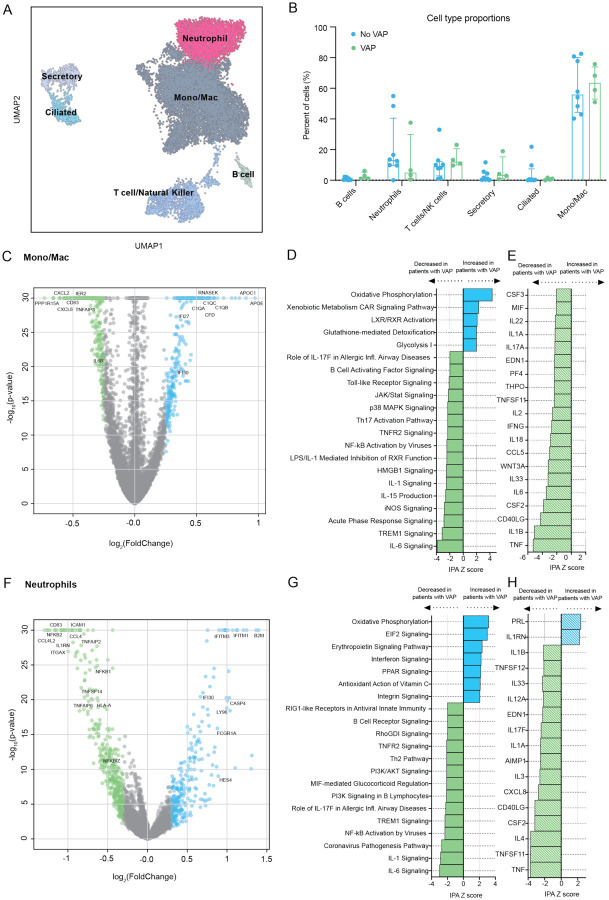
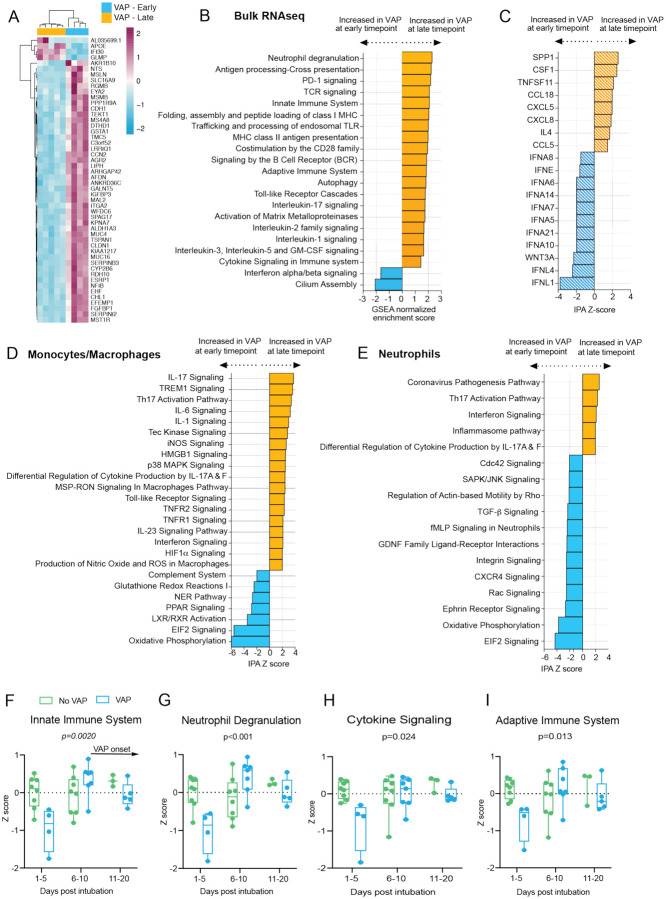
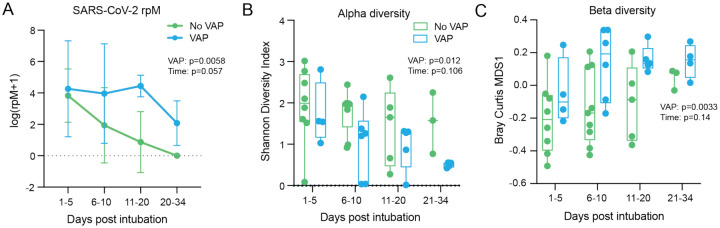
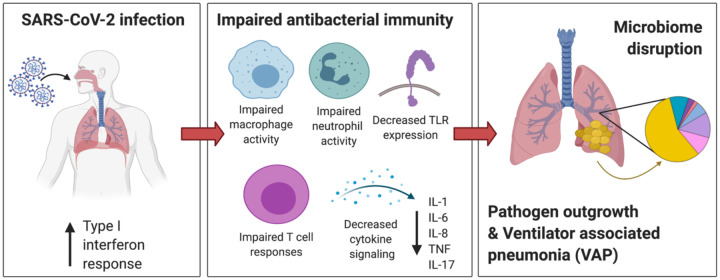
Secondary bacterial infections, including ventilator-associated pneumonia (VAP), lead to worse clinical outcomes and increased mortality following viral respiratory infections including in patients with coronavirus disease 2019 (COVID-19). Using a combination of tracheal aspirate bulk and single-cell RNA sequencing (scRNA-seq) we assessed lower respiratory tract immune responses and microbiome dynamics in 28 COVID-19 patients, 15 of whom developed VAP, and eight critically ill uninfected controls. Two days before VAP onset we observed a transcriptional signature of bacterial infection. Two weeks prior to VAP onset, following intubation, we observed a striking impairment in immune signaling in COVID-19 patients who developed VAP. Longitudinal metatranscriptomic analysis revealed disruption of lung microbiome community composition in patients with VAP, providing a connection between dysregulated immune signaling and outgrowth of opportunistic pathogens. These findings suggest that COVID-19 patients who develop VAP have impaired antibacterial immune defense detectable weeks before secondary infection onset.
Keywords: COVID-19; SARS-CoV-2; VAP; metagenomics; scRNA-seq; secondary bacterial pneumonia.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
