

Longitudinal Measures of Blood Pressure and Subclinical Atrial Arrhythmias: The MESA and the ARIC Study
- PMID: 34014105
- PMCID: PMC8483516
- DOI: 10.1161/JAHA.120.020260
Longitudinal Measures of Blood Pressure and Subclinical Atrial Arrhythmias: The MESA and the ARIC Study
Abstract
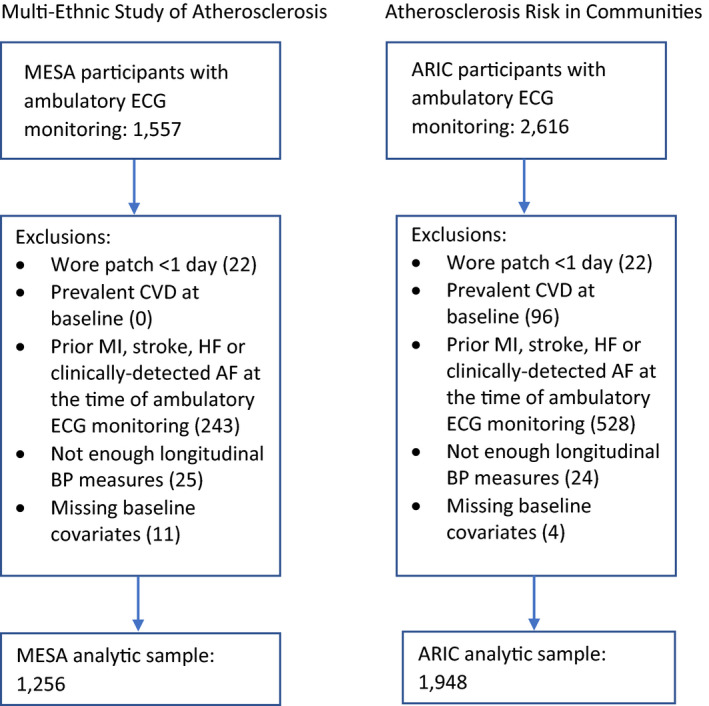
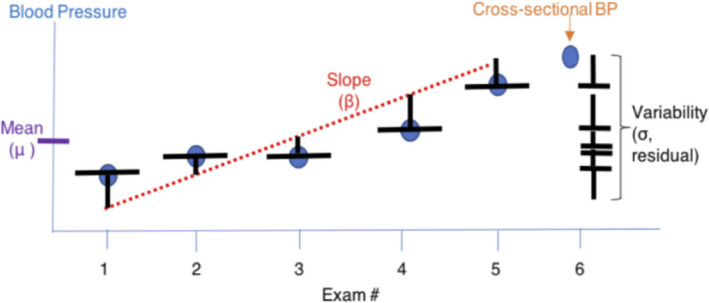
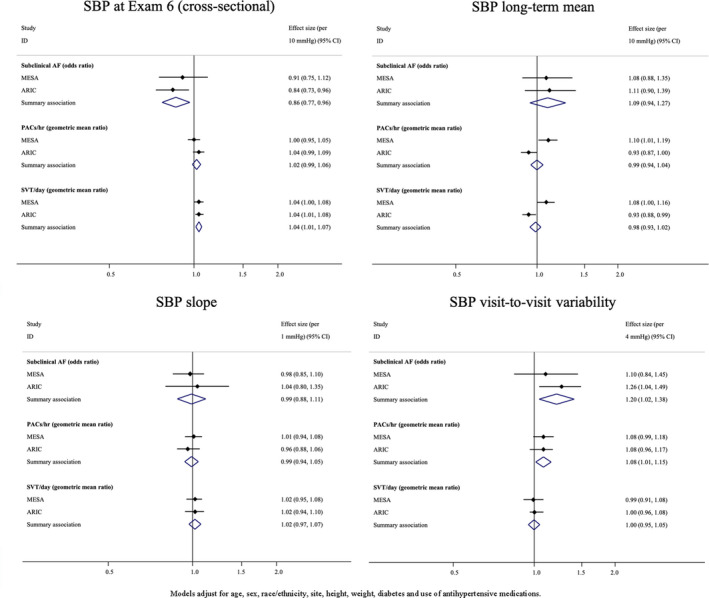
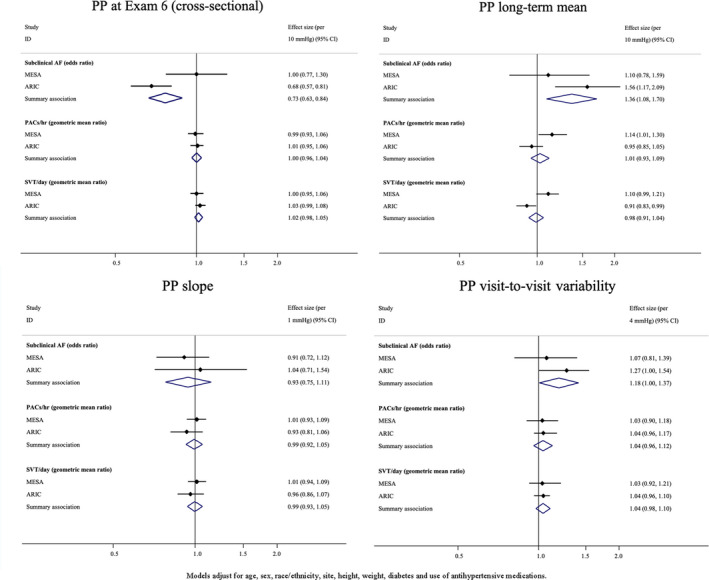
Background High blood pressure (BP) is a well-known risk factor for atrial fibrillation (AF), but a single BP measurement may provide limited information about AF risk in older adults. Methods and Results This study included 1256 MESA (Multi-Ethnic Study of Atherosclerosis) and 1948 ARIC (Atherosclerosis Risk in Communities) study participants who underwent extended ambulatory electrocardiographic monitoring and who were free of clinically detected cardiovascular disease, including AF. Using BP measurements from 6 examinations (2000-2018 in MESA and 1987-2017 in ARIC study), we calculated individual long-term mean, trend, and detrended visit-to-visit variability in systolic BP and pulse pressure for each participant. Outcomes, assessed at examination 6, included subclinical AF and supraventricular ectopy. Results from each study were combined with inverse variance-weighted meta-analysis. At examination 6, the mean age was 73 years in MESA and 79 years in ARIC study, and 4% had subclinical AF. Higher visit-to-visit detrended variability in systolic BP was associated with a greater prevalence of subclinical AF (odds ratio [OR], 1.20; 95% CI, 1.02-1.38) and with more premature atrial contractions/hour (geometric mean ratio, 1.08; 95% CI, 1.01-1.15). For pulse pressure as well, higher visit-to-visit detrended variability was associated with a greater prevalence of AF (OR, 1.18; 95% CI, 1.00-1.37). In addition, higher long-term mean pulse pressure was associated with a greater prevalence of subclinical AF (OR, 1.36; 95% CI, 1.08-1.70). Conclusions Antecedent visit-to-visit variability in systolic BP and pulse pressure, but not current BP, is associated with a higher prevalence of subclinical atrial arrhythmias. Prior longitudinal BP assessment, rather than current BP, may be more helpful in identifying older adults who are at higher risk of atrial arrhythmias.
Keywords: arrhythmia; atrial fibrillation; atrial fibrillation arrhythmia; blood pressure; electrocardiography; older adults.
Conflict of interest statement
Dr Psaty serves on the Steering Committee of the Yale Open Data Access Project, funded by Johnson & Johnson. Dr Floyd has consulted for Shionogi Inc. The remaining authors have no disclosures to report.
Figures
Similar articles
-
Opioid, gabapentinoid, and nonsteroidal anti-inflammatory medication use and the risks of atrial fibrillation and supraventricular ectopy in the Multi-Ethnic Study of Atherosclerosis.Pharmacoepidemiol Drug Saf. 2020 Sep;29(9):1175-1182. doi: 10.1002/pds.5036. Epub 2020 Jun 17. Pharmacoepidemiol Drug Saf. 2020. PMID: 32558036 Free PMC article.
-
Circulating electrolytes and the prevalence of atrial fibrillation and supraventricular ectopy: The Atherosclerosis Risk in Communities (ARIC) study.Nutr Metab Cardiovasc Dis. 2020 Jun 25;30(7):1121-1129. doi: 10.1016/j.numecd.2020.03.010. Epub 2020 Mar 27. Nutr Metab Cardiovasc Dis. 2020. PMID: 32451276 Free PMC article.
-
Fragmented sinoatrial dynamics in the prediction of atrial fibrillation: the Multi-Ethnic Study of Atherosclerosis.Am J Physiol Heart Circ Physiol. 2021 Jan 1;320(1):H256-H271. doi: 10.1152/ajpheart.00421.2020. Epub 2020 Sep 28. Am J Physiol Heart Circ Physiol. 2021. PMID: 32986961 Free PMC article.
-
Atrial Fibrillation Screening During Routine Automated Office, Home, and Ambulatory Blood Pressure Measurement: A Diagnostic Test Accuracy Systematic Review and Meta-Analysis.Hypertension. 2024 Jul;81(7):1477-1488. doi: 10.1161/HYPERTENSIONAHA.123.22563. Epub 2024 Apr 11. Hypertension. 2024. PMID: 38602099
-
Accuracy of automated blood pressure measurements in the presence of atrial fibrillation: systematic review and meta-analysis.J Hum Hypertens. 2019 May;33(5):352-364. doi: 10.1038/s41371-018-0153-z. Epub 2019 Jan 10. J Hum Hypertens. 2019. PMID: 30631126
Cited by
-
Predictors of long-term absence of coronary artery calcium in individuals with high blood pressure: results from the MESA study.Ann Med. 2023 Dec;55(1):2209334. doi: 10.1080/07853890.2023.2209334. Ann Med. 2023. PMID: 37155413 Free PMC article. Clinical Trial.
-
Higher Cumulative Blood Pressure in Midlife Predicts an Increased Risk of Atrial Fibrillation: Evidence From the Atherosclerosis Risk in Communities Study.J Am Heart Assoc. 2023 Dec 19;12(24):e030409. doi: 10.1161/JAHA.123.030409. Epub 2023 Dec 12. J Am Heart Assoc. 2023. PMID: 38084710 Free PMC article.
-
Pulse Pressure and Cardiovascular and Kidney Outcomes by Age in the Chronic Renal Insufficiency Cohort (CRIC).Am J Hypertens. 2025 Jan 16;38(2):129-138. doi: 10.1093/ajh/hpae136. Am J Hypertens. 2025. PMID: 39437324
-
American Heart Association EPI|Lifestyle Scientific Sessions: 2021 Meeting Highlights.J Am Heart Assoc. 2022 Mar;11(5):e024765. doi: 10.1161/JAHA.121.024765. Epub 2022 Feb 18. J Am Heart Assoc. 2022. PMID: 35179039 Free PMC article. No abstract available.
-
Blood pressure fragmentation as a new measure of blood pressure variability: association with predictors of cardiac surgery outcomes.Front Physiol. 2024 Feb 9;15:1277592. doi: 10.3389/fphys.2024.1277592. eCollection 2024. Front Physiol. 2024. PMID: 38405117 Free PMC article.
References
-
- Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, D'Agostino RB, Murabito JM, Kannel WB, Benjamin EJ. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham heart study. Circulation. 2003;107:2920–2925. DOI: 10.1161/01.CIR.0000072767.89944.6E. - DOI - PubMed
-
- Piccini JP, Hammill BG, Sinner MF, Jensen PN, Hernandez AF, Heckbert SR, Benjamin EJ, Curtis LH. Incidence and prevalence of atrial fibrillation and associated mortality among Medicare beneficiaries, 1993–2007. Circ Cardiovasc Qual Outcomes. 2012;5:85–93. DOI: 10.1161/CIRCOUTCOMES.111.962688. - DOI - PMC - PubMed
-
- Tielemans SM, Geleijnse JM, Menotti A, Boshuizen HC, Soedamah‐Muthu SS, Jacobs DR Jr, Blackburn H, Kromhout D. Ten‐year blood pressure trajectories, cardiovascular mortality, and life years lost in 2 extinction cohorts: the Minnesota business and professional men study and the Zutphen study. J Am Heart Assoc. 2015;4:e001378. DOI: 10.1161/JAHA.114.001378. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201500003C/HL/NHLBI NIH HHS/United States
- 75N90020D00002/CL/CLC NIH HHS/United States
- 75N96020D00002/ES/NIEHS NIH HHS/United States
- 75N93020D00002/AI/NIAID NIH HHS/United States
- T32 HL007828/HL/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- N01 HC095169/HC/NHLBI NIH HHS/United States
- 75N95020D00005/DA/NIDA NIH HHS/United States
- HHSN268201500003I/HL/NHLBI NIH HHS/United States
- 75N99020D00007/OF/ORFDO NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095167/HC/NHLBI NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- 75N95020D00003/DA/NIDA NIH HHS/United States
- R01 HL126637/HL/NHLBI NIH HHS/United States
- N01 HC095168/HC/NHLBI NIH HHS/United States
- 75N99020D00003/OF/ORFDO NIH HHS/United States
- 75N95020D00002/DA/NIDA NIH HHS/United States
- R01 HL142599/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- 75N90020D00003/CL/CLC NIH HHS/United States
- 75N96020D00003/ES/NIEHS NIH HHS/United States
- 75N99020D00002/OF/ORFDO NIH HHS/United States
- HHSN268201700002C/HL/NHLBI NIH HHS/United States
- HHSN268201700001I/HL/NHLBI NIH HHS/United States
- 75N99020D00006/OF/ORFDO NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- HHSN268201700004I/HL/NHLBI NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- 75N95020D00007/DA/NIDA NIH HHS/United States
- 75N92021D00006/HL/NHLBI NIH HHS/United States
- HHSN268201700005C/HL/NHLBI NIH HHS/United States
- HHSN268201700001C/HL/NHLBI NIH HHS/United States
- 75N99020D00005/OF/ORFDO NIH HHS/United States
- N01 HC095166/HC/NHLBI NIH HHS/United States
- HHSN268201700003C/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- HHSN268201700004C/HL/NHLBI NIH HHS/United States
- HHSN268201700002I/HL/NHLBI NIH HHS/United States
- HHSN268201700005I/HL/NHLBI NIH HHS/United States
- 75N98020D00007/OD/NIH HHS/United States
- HHSN268201700003I/HL/NHLBI NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- 75N95020D00004/DA/NIDA NIH HHS/United States
- R01 HL127659/HL/NHLBI NIH HHS/United States
- 75N99020D00004/OF/ORFDO NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
