

Cardiovascular and Kidney Outcomes Across the Glycemic Spectrum: Insights From the UK Biobank
- PMID: 34015477
- PMCID: PMC8324525
- DOI: 10.1016/j.jacc.2021.05.004
Cardiovascular and Kidney Outcomes Across the Glycemic Spectrum: Insights From the UK Biobank
Abstract
Background: Treatment guidelines for prediabetes primarily focus on glycemic control and lifestyle management. Few evidence-based cardiovascular and kidney risk-reduction strategies are available in this population.
Objectives: This study sought to characterize cardiovascular and kidney outcomes across the glycemic spectrum.
Methods: Among participants in the UK Biobank without prevalent type 1 diabetes, cardiovascular disease, or kidney disease, Cox models tested the association of glycemic exposures (type 2 diabetes [T2D], prediabetes, normoglycemia) with outcomes (atherosclerotic cardiovascular disease [ASCVD], chronic kidney disease [CKD], and heart failure), adjusting for demographic, lifestyle, and cardiometabolic risk factors.
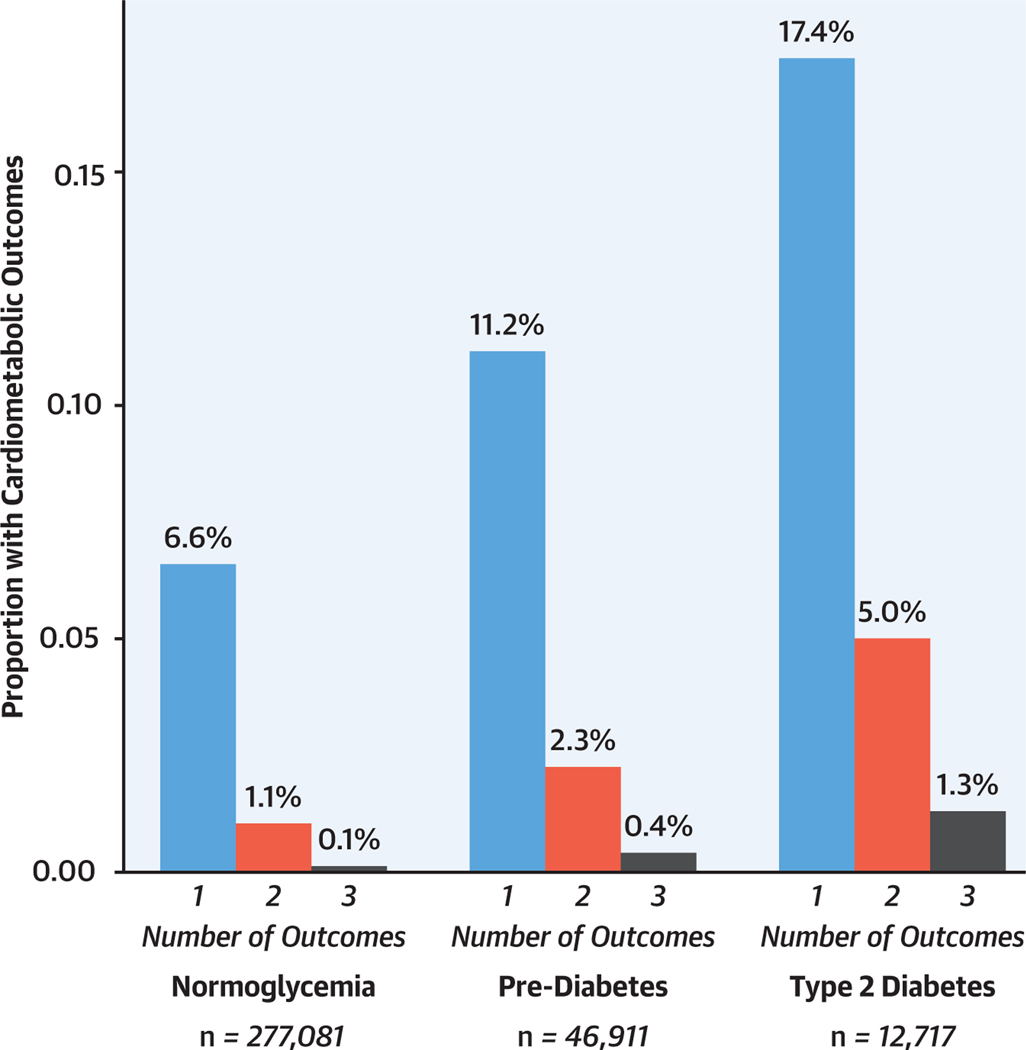
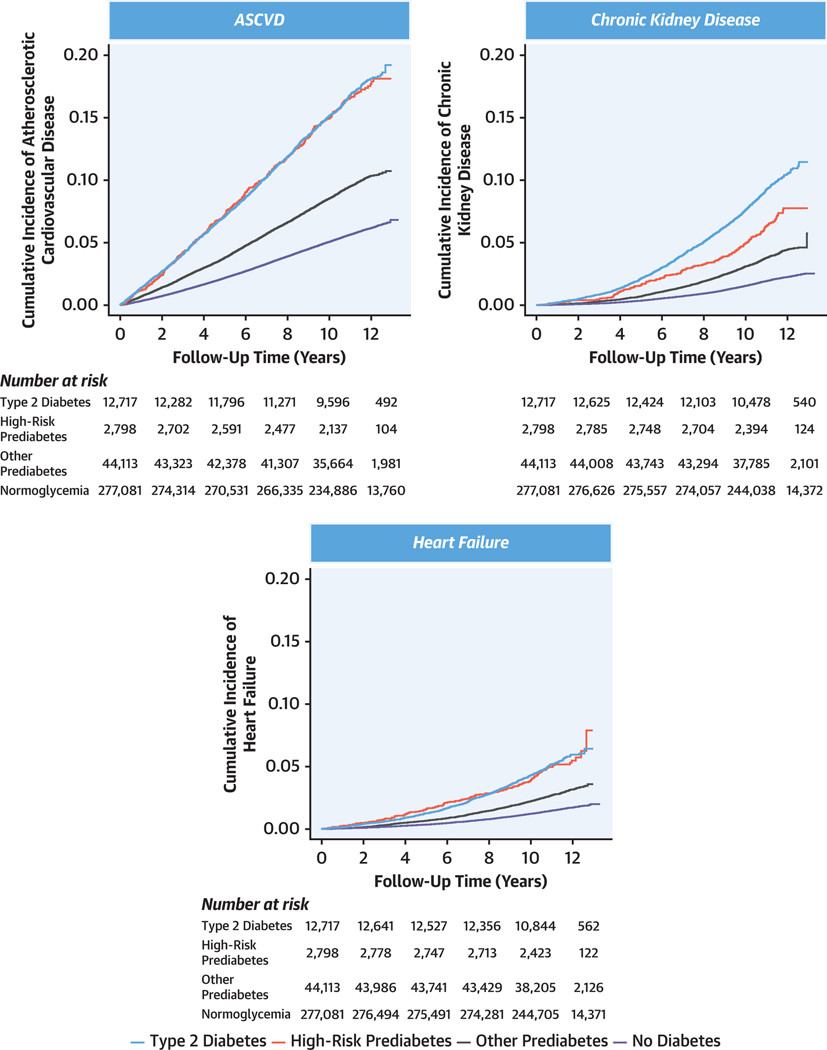
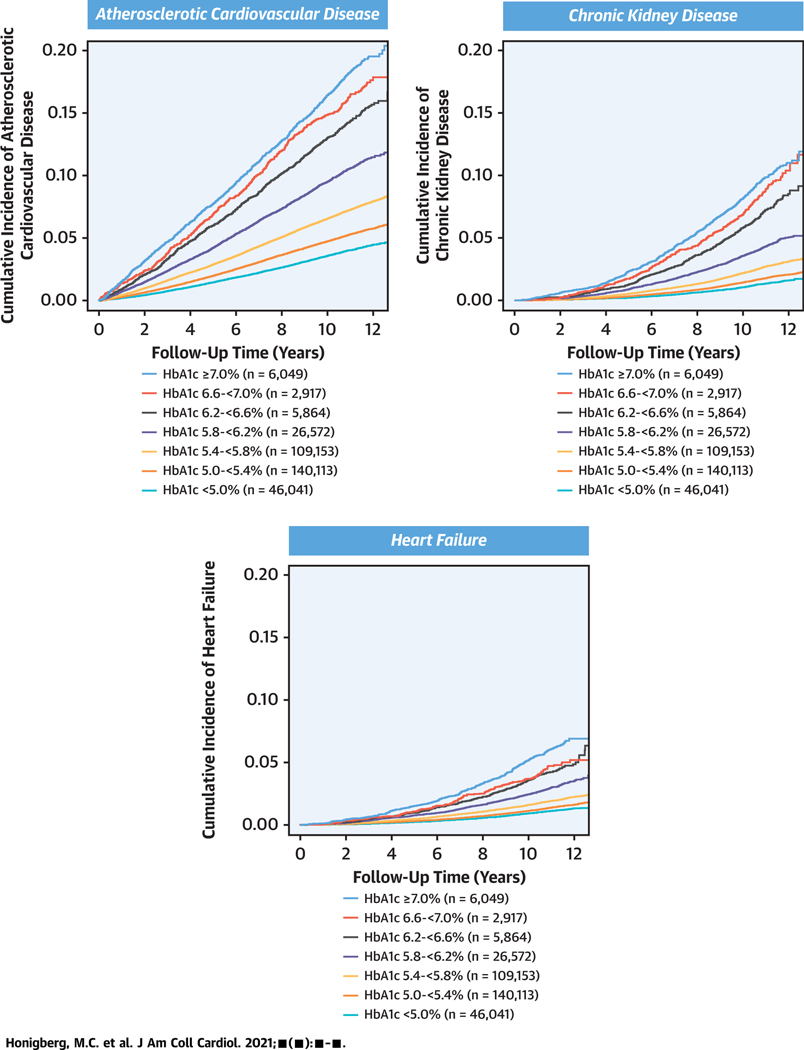
Results: Among 336,709 individuals (mean age: 56.3 years, 55.4% female), 46,911 (13.9%) had prediabetes and 12,717 (3.8%) had T2D. Over median follow-up of 11.1 years, 6,476 (13.8%) individuals with prediabetes developed ≥1 incident outcome, of whom only 802 (12.4%) developed T2D prior to an incident diagnosis. Prediabetes and T2D were independently associated with ASCVD (prediabetes: adjusted HR [aHR]: 1.11; 95% CI: 1.08-1.15; P < 0.001; T2D: aHR: 1.44; 95% CI: 1.37-1.51; P < 0.001), CKD (prediabetes: aHR: 1.08; 95% CI: 1.02-1.14; P < 0.001; T2D: aHR: 1.57; 95% CI: 1.46-1.69; P < 0.001), and heart failure (prediabetes: aHR: 1.07; 95% CI: 1.01-1.14; P = 0.03; T2D: aHR: 1.25; 95% CI: 1.14-1.37; P < 0.001). Compared with hemoglobin A1c (HbA1c) <5.0%, covariate-adjusted risks increased significantly for ASCVD above HbA1c of 5.4%, CKD above HbA1c of 6.2%, and heart failure above HbA1c of 7.0%.
Conclusions: Prediabetes and T2D were associated with ASCVD, CKD, and heart failure, but a substantial gradient of risk was observed across HbA1c levels below the threshold for diabetes. These findings highlight the need to design risk-reduction strategies across the glycemic spectrum.
Keywords: atherosclerotic cardiovascular disease; heart failure; prediabetes; prevention; type 2 diabetes.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Honigberg is supported by a grant from the National Heart, Lung, and Blood Institute (T32HL094301-07). Dr Natarajan is supported by grants from the National Heart, Lung, and Blood Institute (R01HL142711, R01HL148050, R01HL148565, R01HL151283), Fondation Leducq (TNE-18CVD04), and a Hassenfeld Scholar Award from Massachusetts General Hospital; has received grant support from Amgen, Apple, Boston Scientific, and Novartis; has received personal fees from Apple, Blackstone Life Sciences, Genentech, and Novartis; and Dr Natarajan’s spouse has been employed by Vertex, all unrelated to the present work. Dr Vaduganathan has received research grant support or served on advisory boards for American Regent, Amgen, AstraZeneca, Bayer AG, Baxter Healthcare, Boehringer Ingelheim, Cytokinetics, Lexicon Pharmaceuticals, and Relypsa; has had speaking engagements with Novartis and Roche Diagnostics; and has participated on clinical endpoint committees for studies sponsored by Galmed and Novartis. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Closing the Glycemic Divide: The Time for Preventive Cardiology Is Now.J Am Coll Cardiol. 2021 Aug 3;78(5):465-467. doi: 10.1016/j.jacc.2021.05.040. J Am Coll Cardiol. 2021. PMID: 34325835 No abstract available.
References
-
- Dinesh Shah A, Langenberg C, Rapsomaniki E, et al. Type 2 diabetes and incidence of a wide range of cardiovascular diseases: a cohort study in 1–9 million people. Lancet 2015;385 suppl 1:S86. - PubMed
-
- Rawshani A, Franzén S, Eliasson B, et al. Mortality and cardiovascular disease in type 1 and type 2 diabetes. N Engl J Med 2017;376(15):1407–18. - PubMed
-
- Rawshani A, Franzén S, Sattar N, et al. Risk factors, mortality, and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2018; 379(7):633–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
