

Burden of Clostridioides difficile infection (CDI) - a systematic review of the epidemiology of primary and recurrent CDI
- PMID: 34016040
- PMCID: PMC8135979
- DOI: 10.1186/s12879-021-06147-y
Burden of Clostridioides difficile infection (CDI) - a systematic review of the epidemiology of primary and recurrent CDI
Abstract
Background: Clostridioides difficile is a Gram-positive anaerobic bacterium, which causes Clostridioides difficile infection (CDI). It has been recognised as a leading cause of healthcare-associated infections and a considerable threat to public health globally. This systematic literature review (SLR) summarises the current evidence on the epidemiology and clinical burden of CDI.
Methods: A SLR was conducted to identify CDI and recurrent CDI (rCDI) epidemiology studies, to evaluate patient and disease characteristics, incidence rates, epidemiological findings and risk factors. Embase, MEDLINE and the Cochrane Library databases were searched for English articles from 2009 to 2019. Included territories were the United Kingdom, France, Germany, Italy, Spain, Poland, US, Canada, Australia, Japan and China.
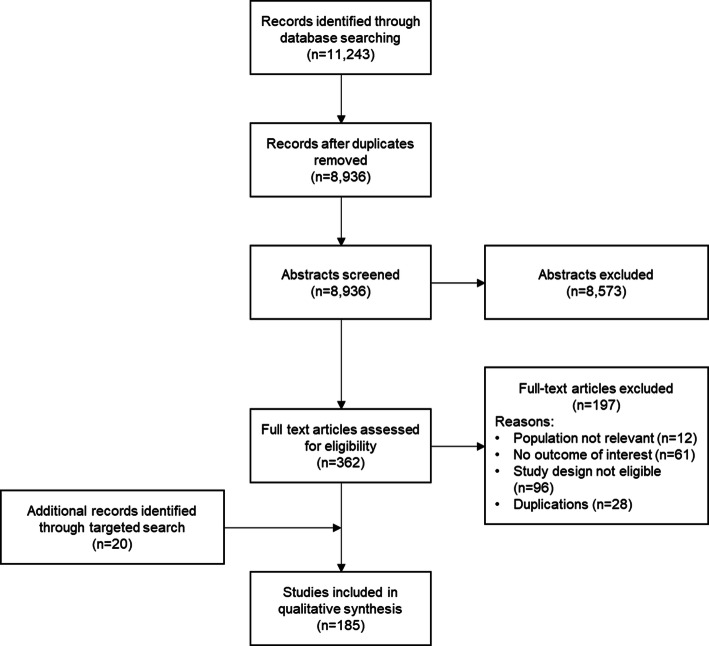
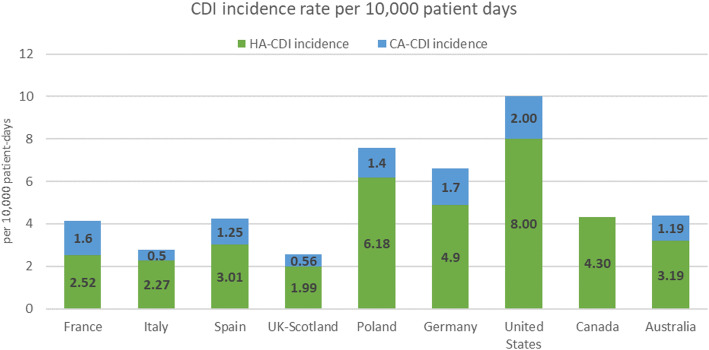
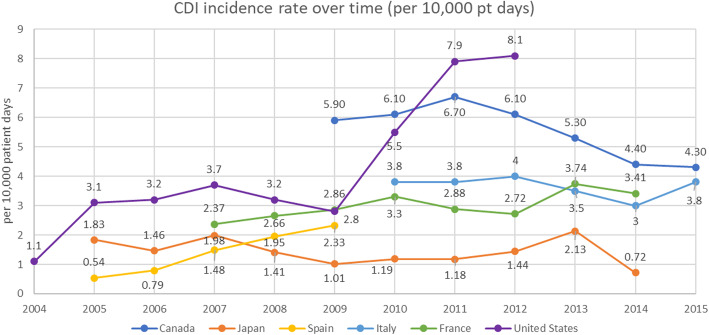
Results: Of 11,243 studies identified, 165 fulfilled the selection criteria. An additional 20 studies were identified through targeted review of grey literature. The most widely reported findings were incidence and risk factors for CDI and rCDI. Among key studies reporting both healthcare-associated (HA-CDI) and community-associated CDI (CA-CDI) incidence rates for each country of interest, incidence rates per 10,000 patient days in the US were 8.00 and 2.00 for HA-CDI and CA-CDI, respectively. The highest incidence in Europe was reported in Poland (HA-CDI: 6.18 per 10,000 patient days, CA-CDI: 1.4 per 10,000 patient days), the lowest from the UK, at 1.99 per 10,000 patient days and 0.56 per 10,000 patient days for HA-CDI and CA-CDI, respectively. No clear trend for incidence over time emerged, with most countries reporting stable rates but some either a decrease or increase. Rates of recurrent CDI varied based on geographical setting. The rate of recurrence was lower in community-associated disease compared to healthcare-associated disease. Independent CDI risk factors identified common to both initial CDI and recurrent CDI included increasing age, antibiotic use, recent hospitalisation, and proton pump inhibitor (PPI) use. In addition, leukocyte count, length of hospital stays, and Charlson comorbidity index score featured as statistically significant risk factors for recurrent CDI, but these are not reported among the most common statistically significant risk factors for initial CDI.
Conclusions: Despite considerable heterogeneity, evidence suggests substantial incidence of recurrent and primary CDI, even after considerable efforts in the last decade.
Keywords: Antibiotic resistance; Antimicrobial stewardship; Clostridioides difficile; Epidemiology; Recurrent Clostridioides difficile; Risk factors.
Conflict of interest statement
FLA is employed by Ferring Pharmaceuticals, which is conducting research in the microbiome field. EF and MM are full-time employees of IQVIA and acted as consultants for this study funded by Ferring Pharmaceuticals.
Figures
References
-
- Jones AM, Kuijper EJ, Wilcox MH. Clostridium difficile: a European perspective. J Inf Secur. 2013;66(2):115–128. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
