

The age again in the eye of the COVID-19 storm: evidence-based decision making
- PMID: 34016150
- PMCID: PMC8134808
- DOI: 10.1186/s12979-021-00237-w
The age again in the eye of the COVID-19 storm: evidence-based decision making
Abstract
Background: One hundred fifty million contagions, more than 3 million deaths and little more than 1 year of COVID-19 have changed our lives and our health management systems forever. Ageing is known to be one of the significant determinants for COVID-19 severity. Two main reasons underlie this: immunosenescence and age correlation with main COVID-19 comorbidities such as hypertension or dyslipidaemia. This study has two aims. The first is to obtain cut-off points for laboratory parameters that can help us in clinical decision-making. The second one is to analyse the effect of pandemic lockdown on epidemiological, clinical, and laboratory parameters concerning the severity of the COVID-19. For these purposes, 257 of SARSCoV2 inpatients during pandemic confinement were included in this study. Moreover, 584 case records from a previously analysed series, were compared with the present study data.
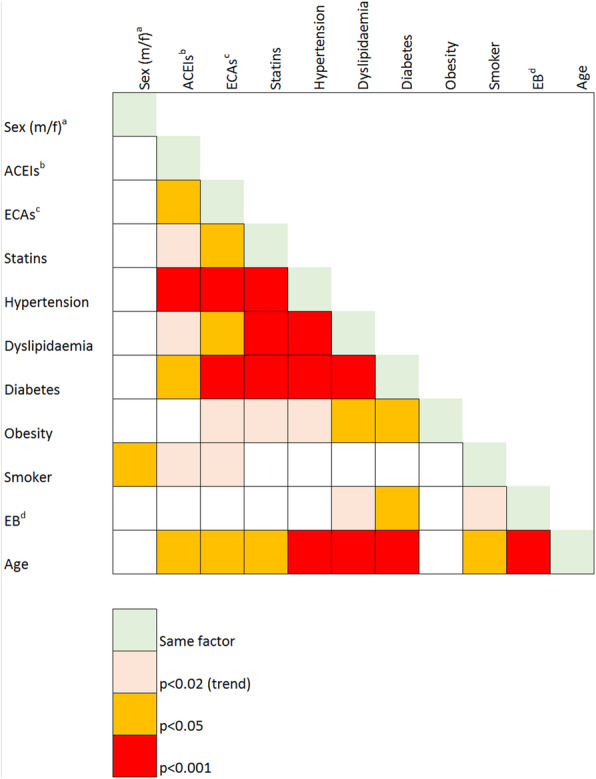
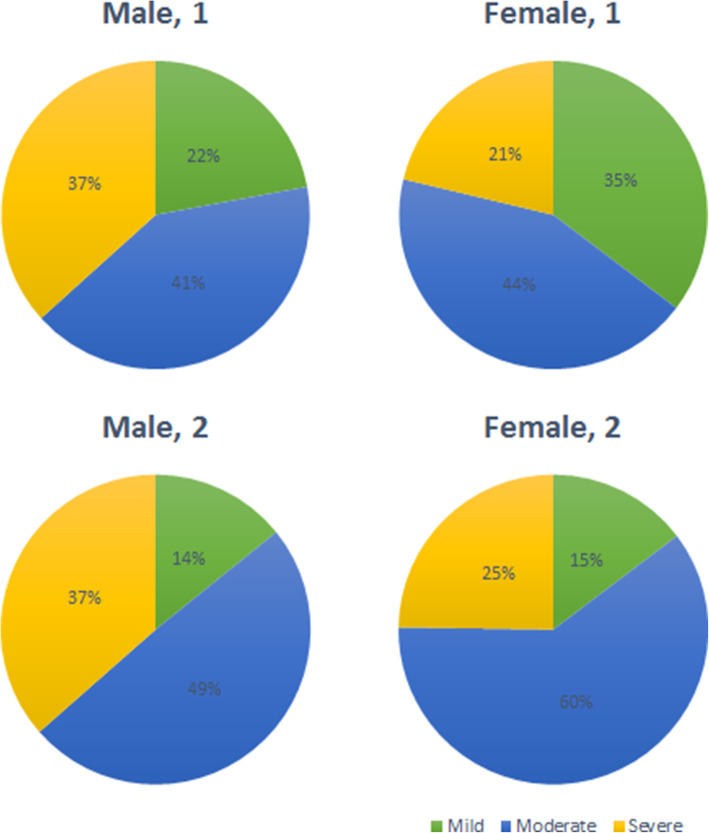
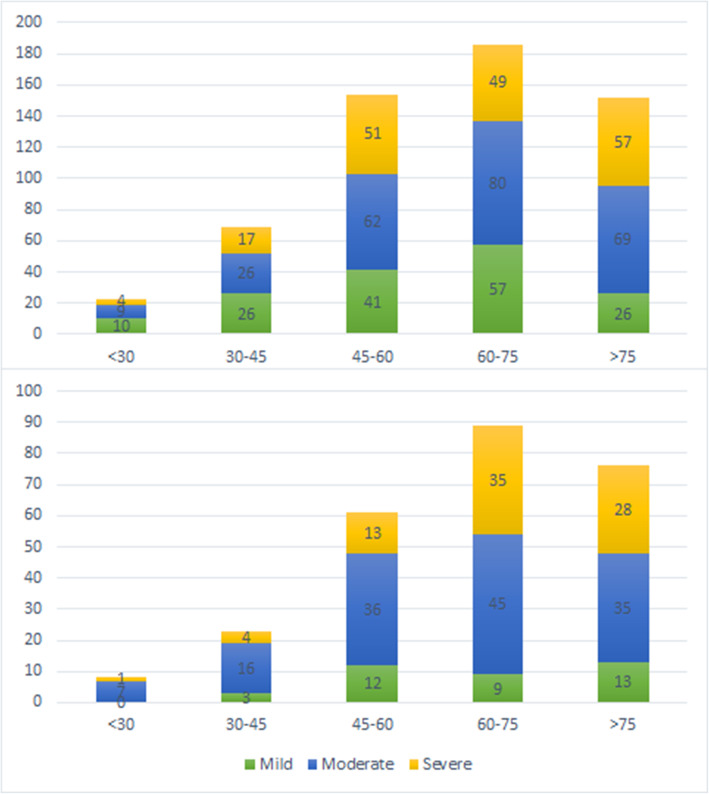
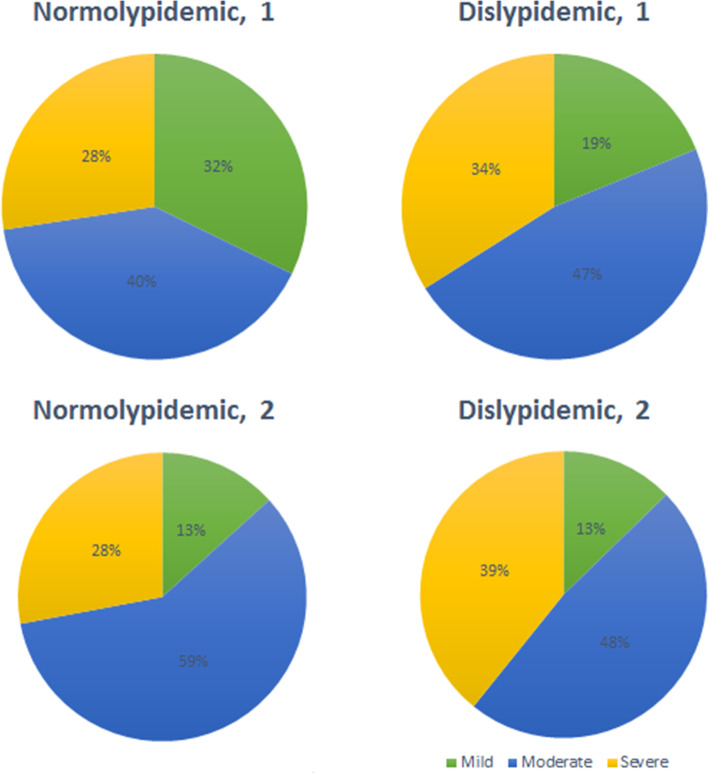
Results: Concerning the characteristics of lockdown series, mild cases accounted for 14.4, 54.1% were moderate and 31.5%, severe. There were 32.5% of home contagions, 26.3% community transmissions, 22.5% nursing home contagions, and 8.8% corresponding to frontline worker contagions regarding epidemiological features. Age > 60 and male sex are hereby confirmed as severity determinants. Equally, higher severity was significantly associated with higher IL6, CRP, ferritin, LDH, and leukocyte counts, and a lower percentage of lymphocyte, CD4 and CD8 count. Comparing this cohort with a previous 584-cases series, mild cases were less than those analysed in the first moment of the pandemic and dyslipidaemia became more frequent than before. IL-6, CRP and LDH values above 69 pg/mL, 97 mg/L and 328 U/L respectively, as well as a CD4 T-cell count below 535 cells/μL, were the best cut-offs predicting severity since these parameters offered reliable areas under the curve.
Conclusion: Age and sex together with selected laboratory parameters on admission can help us predict COVID-19 severity and, therefore, make clinical and resource management decisions. Demographic features associated with lockdown might affect the homogeneity of the data and the robustness of the results.
Keywords: Area under the curve; COVID-19; Cut-off points; Immunity; Immunosenescence; Lockdown; Lymphocytes; Renin-angiotensin-aldosterone system inhibitors; Severe acute respiratory syndrome coronavirus 2.
Conflict of interest statement
The authors stated no conflicts of interest.
Figures
References
-
- COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). https://coronavirus.jhu.edu/map.html. Accessed 3 May 2021.
-
- Riveiro-Barciela M, Labrador-Horrillo M, Camps-Relats L, González-Sans D, Ventura-Cots M, Terrones-Peinador M, Nuñez-Conde A, Martínez-Gallo M, Hernández M, Antón A, González A, Pujol-Borrell R, Martínez-Valle F. Simple predictive models identify patients with COVID-19 pneumonia and poor prognosis. PLoS One. 2020;15(12):e0244627. doi: 10.1371/journal.pone.0244627. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
