

Latent Autoimmune Diabetes of Adults (LADA) Is Likely to Represent a Mixed Population of Autoimmune (Type 1) and Nonautoimmune (Type 2) Diabetes
- PMID: 34016607
- PMCID: PMC8247509
- DOI: 10.2337/dc20-2834
Latent Autoimmune Diabetes of Adults (LADA) Is Likely to Represent a Mixed Population of Autoimmune (Type 1) and Nonautoimmune (Type 2) Diabetes
Abstract
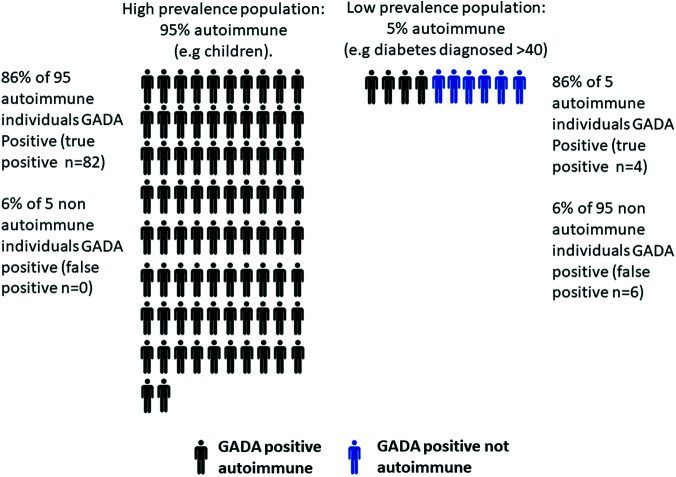
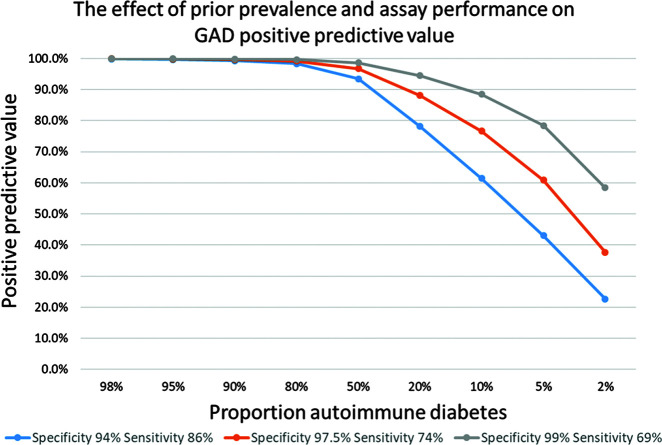
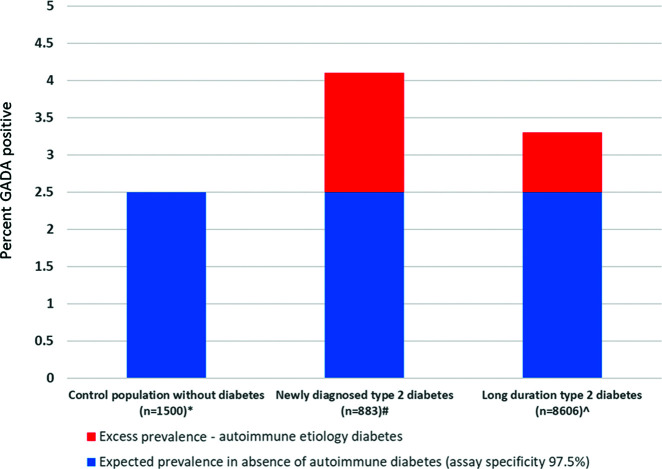
Latent autoimmune diabetes of adults (LADA) is typically defined as a new diabetes diagnosis after 35 years of age, presenting with clinical features of type 2 diabetes, in whom a type 1 diabetes-associated islet autoantibody is detected. Identifying autoimmune diabetes is important since the prognosis and optimal therapy differ. However, the existing LADA definition identifies a group with clinical and genetic features intermediate between typical type 1 and type 2 diabetes. It is unclear whether this is due to 1) true autoimmune diabetes with a milder phenotype at older onset ages that initially appears similar to type 2 diabetes but later requires insulin, 2) a disease syndrome where the pathophysiologies of type 1 and type 2 diabetes are both present in each patient, or 3) a heterogeneous group resulting from difficulties in classification. Herein, we suggest that difficulties in classification are a major component resulting from defining LADA using a diagnostic test-islet autoantibody measurement-with imperfect specificity applied in low-prevalence populations. This yields a heterogeneous group of true positives (autoimmune type 1 diabetes) and false positives (nonautoimmune type 2 diabetes). For clinicians, this means that islet autoantibody testing should not be undertaken in patients who do not have clinical features suggestive of autoimmune diabetes: in an adult without clinical features of type 1 diabetes, it is likely that a single positive antibody will represent a false-positive result. This is in contrast to patients with features suggestive of type 1 diabetes, where false-positive results will be rare. For researchers, this means that current definitions of LADA are not appropriate for the study of autoimmune diabetes in later life. Approaches that increase test specificity, or prior likelihood of autoimmune diabetes, are needed to avoid inclusion of participants who have nonautoimmune (type 2) diabetes. Improved classification will allow improved assignment of prognosis and therapy as well as an improved cohort in which to analyze and better understand the detailed pathophysiological components acting at onset and during disease progression in late-onset autoimmune diabetes.
© 2021 by the American Diabetes Association.
Figures
References
-
- Buzzetti R, Zampetti S, Maddaloni E. Adult-onset autoimmune diabetes: current knowledge and implications for management. Nat Rev Endocrinol 2017;13:674–686 - PubMed
-
- World Health Organization . Classification of diabetes mellitus. Geneva, World Health Organization, 2019
-
- Bottazzo GF, Florin-Christensen A, Doniach D. Islet-cell antibodies in diabetes mellitus with autoimmune polyendocrine deficiencies. Lancet 1974;2:1279–1283 - PubMed
-
- Lendrum R, Walker G, Gamble DR. Islet-cell antibodies in juvenile diabetes mellitus of recent onset. Lancet 1975;1:880–882 - PubMed
-
- Groop LC, Bottazzo GF, Doniach D. Islet cell antibodies identify latent type I diabetes in patients aged 35-75 years at diagnosis. Diabetes 1986;35:237–241 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
