

Comparing Pediatric Gastroenteritis Emergency Department Care in Canada and the United States
- PMID: 34016656
- PMCID: PMC8785749
- DOI: 10.1542/peds.2020-030890
Comparing Pediatric Gastroenteritis Emergency Department Care in Canada and the United States
Abstract
Background: Between-country variation in health care resource use and its impact on outcomes in acute care settings have been challenging to disentangle from illness severity by using administrative data.
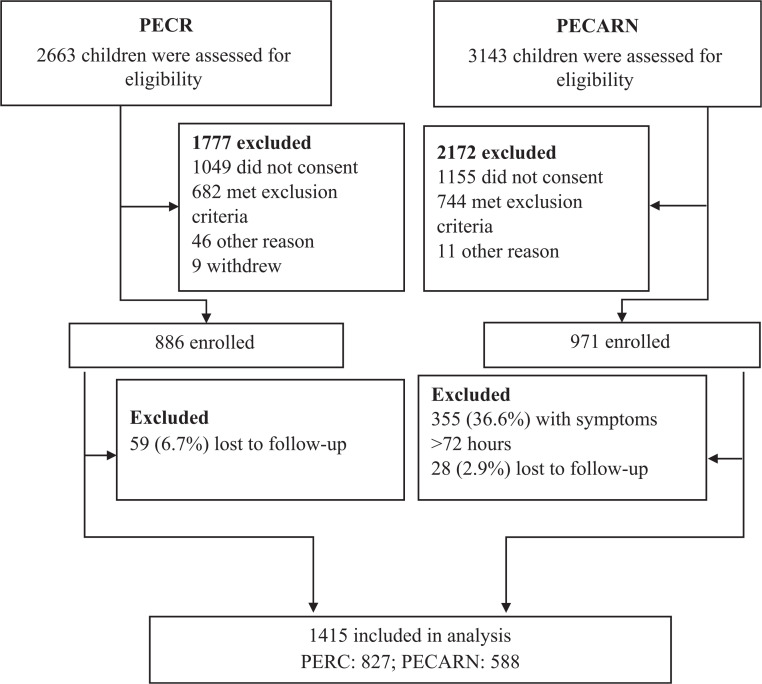
Methods: We conducted a preplanned analysis employing patient-level emergency department (ED) data from children enrolled in 2 previously conducted clinical trials. Participants aged 3 to <48 months with <72 hours of gastroenteritis were recruited in pediatric EDs in the United States (N = 10 sites; 588 participants) and Canada (N = 6 sites; 827 participants). The primary outcome was an unscheduled health care provider visit within 7 days; the secondary outcomes were intravenous fluid administration and hospitalization at or within 7 days of the index visit.
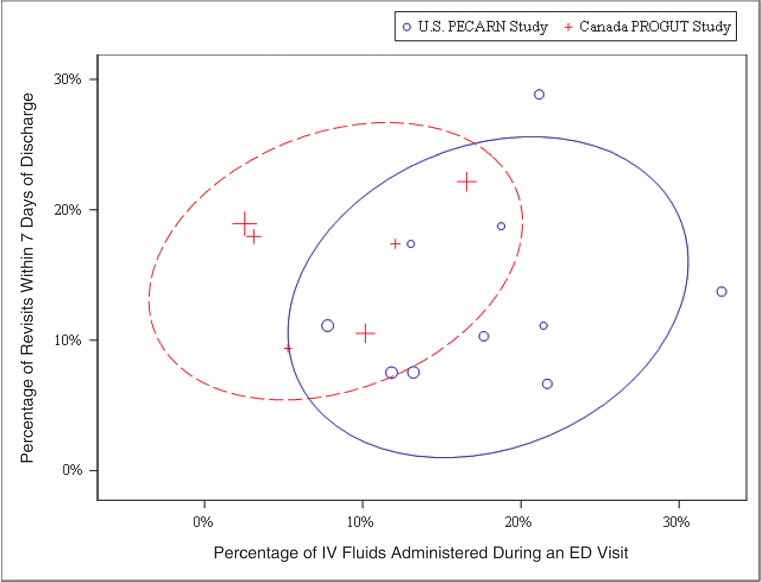
Results: In adjusted analysis, unscheduled revisits within 7 days did not differ (adjusted odds ratio [aOR]: 0.72; 95% confidence interval (CI): 0.50 to 1.02). At the index ED visit, although participants in Canada were assessed as being more dehydrated, intravenous fluids were administered more frequently in the United States (aOR: 4.6; 95% CI: 2.9 to 7.1). Intravenous fluid administration rates did not differ after enrollment (aOR: 1.4; 95% CI: 0.7 to 2.8; US cohort with Canadian as referent). Overall, intravenous rehydration was higher in the United States (aOR: 3.8; 95% CI: 2.5 to 5.7). Although hospitalization rates during the 7 days after enrollment (aOR: 1.1; 95% CI: 0.4 to 2.6) did not differ, hospitalization at the index visit was more common in the United States (3.9% vs 2.3%; aOR: 3.2; 95% CI: 1.6 to 6.8).
Conclusions: Among children with gastroenteritis and similar disease severity, revisit rates were similar in our 2 study cohorts, despite lower rates of intravenous rehydration and hospitalization in Canadian-based EDs.
Trial registration: ClinicalTrials.gov NCT01773967 NCT01853124.
Copyright © 2021 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Comment in
-
Gastroenteritis Care in the US and Canada: Can Comparative Analysis Improve Resource Use?Pediatrics. 2021 Jun;147(6):e2021050436. doi: 10.1542/peds.2021-050436. Epub 2021 May 20. Pediatrics. 2021. PMID: 34016657 No abstract available.
References
-
- World Health Organization. Health expenditure profile. Available at: http://apps.who.int/nha/database/Country_Profile/Index/en. Accessed March 22, 2020
-
- Papanicolas I, Woskie LR, Jha AK. Health care spending in the United States and other high-income countries. [published correction appears in JAMA. 2018;319(17):1824]. JAMA. 2018;319(10):1024–1039 - PubMed
-
- GBD 2015 Healthcare Access and Quality Collaborators. Electronic address: cjlm@uw.edu; GBD 2015 Healthcare Access and Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet. 2017;390(10091):231–266 - PMC - PubMed
-
- McDermott KW, Stocks C, Freeman WJ. Overview of Pediatric Emergency Department Visits, 2015: Statistical Brief #242. Rockville, MD: Agency for Healthcare Research and Quality; 2018 - PubMed
-
- Jamal A, Finkelstein Y, Kuppermann N, et al. ; Pediatric Emergency Research Networks . Pharmacotherapy in bronchiolitis at discharge from emergency departments within the Pediatric Emergency Research Networks: a retrospective analysis. Lancet Child Adolesc Health. 2019;3(8):539–547 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
