

Improving detection and management of familial hypercholesterolaemia in Australian general practice
- PMID: 34016696
- PMCID: PMC8292556
- DOI: 10.1136/heartjnl-2020-318813
Improving detection and management of familial hypercholesterolaemia in Australian general practice
Abstract
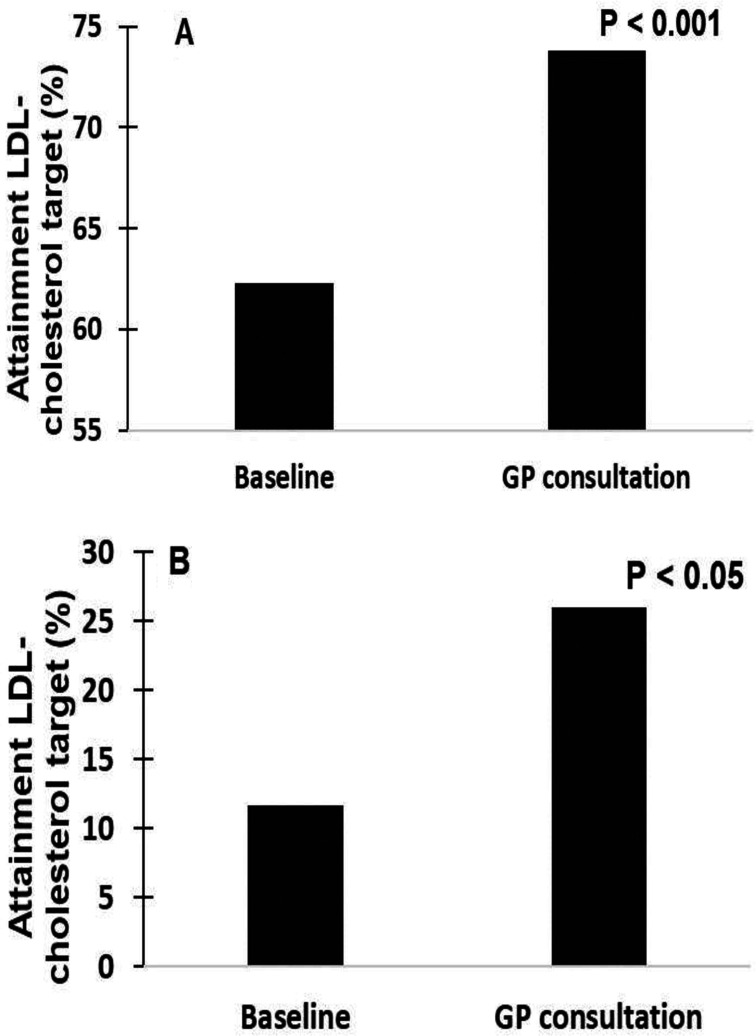
Objective: Familial hypercholesterolaemia (FH) is characterised by elevated low-density lipoprotein (LDL)-cholesterol and increased risk of cardiovascular disease. However, FH remains substantially underdiagnosed and undertreated. We employed a two-stage pragmatic approach to identify and manage patients with FH in primary healthcare.
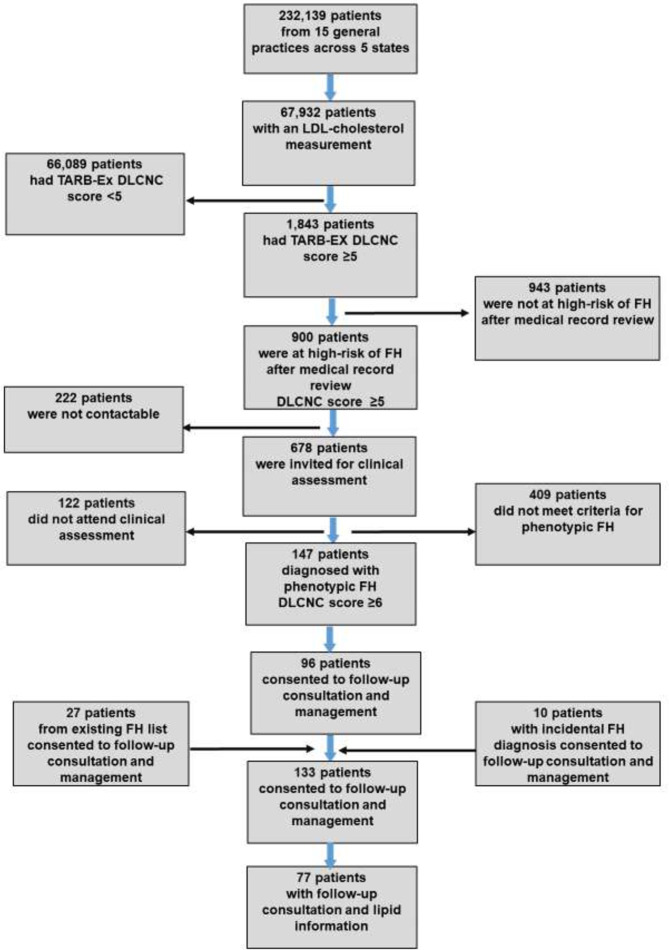
Methods: Medical records for 232 139 patients who attended 15 general practices at least once in the previous 2 years across five Australian States were first screened for potential risk of FH using an electronic tool (TARB-Ex) and confirmed by general practitioner (GP) clinical assessment based on phenotypic Dutch Lipid Clinic Network Criteria (DLCNC) score. Follow-up GP consultation and management was provided for patients with phenotypic FH.
Results:
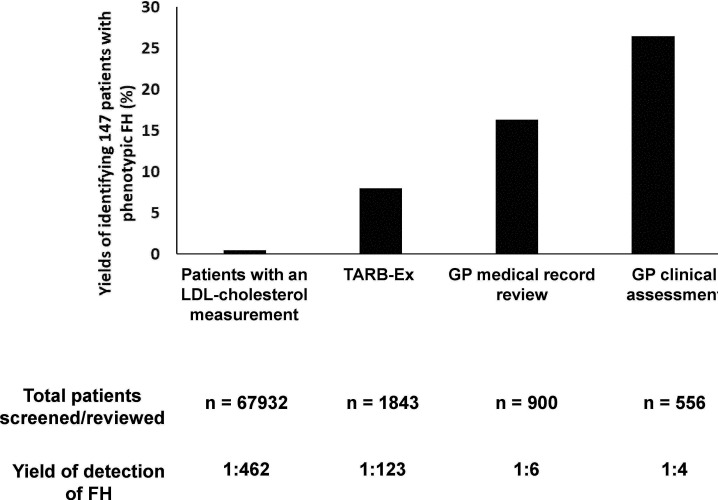
A total of 1843 patients were identified by TARB-Ex as at potential risk of FH (DLCNC score ≥5). After GP medical record review, 900 of these patients (49%) were confirmed with DLCNC score ≥5 and classified as high-risk of FH. From 556 patients subsequently clinically assessed by GPs, 147 (26%) were diagnosed with phenotypic FH (DLCNC score
Conclusions: A pragmatic approach integrating electronic medical record tools and clinical GP follow-up consultation is a feasible method to identify and better manage patients with FH in the primary healthcare setting.
Trial registration number: 12616000630415.
Keywords: atherosclerosis; delivery of healthcare; electronic health records; global burden of disease; hyperlipidemias.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: TB has received honoraria for lectures or research grants from Amgen and Sanofi. DAR has received research grants from Sanofi and WA Department of Health, and travel and accommodation support from Amgen. GW has received honoraria for lectures and advisory boards or research grants from Amgen, Arrowhead, AstraZeneca, Esperion, Kowa, Novartis, Regeneron and Sanofi.
Figures
References
-
- Borén J, Chapman MJ, Krauss RM, et al. . Low-Density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European atherosclerosis Society consensus panel. Eur Heart J 2020;41:2313–30. 10.1093/eurheartj/ehz962 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous