

Efficacy and safety of a novel dosing strategy for ruxolitinib in the treatment of patients with myelofibrosis and anemia: the REALISE phase 2 study
- PMID: 34017073
- PMCID: PMC8632662
- DOI: 10.1038/s41375-021-01261-x
Efficacy and safety of a novel dosing strategy for ruxolitinib in the treatment of patients with myelofibrosis and anemia: the REALISE phase 2 study
Erratum in
-
Correction: Efficacy and safety of a novel dosing strategy for ruxolitinib in the treatment of patients with myelofibrosis and anemia: the REALISE phase 2 study.Leukemia. 2021 Dec;35(12):3626. doi: 10.1038/s41375-021-01396-x. Leukemia. 2021. PMID: 34475521 Free PMC article. No abstract available.
Abstract
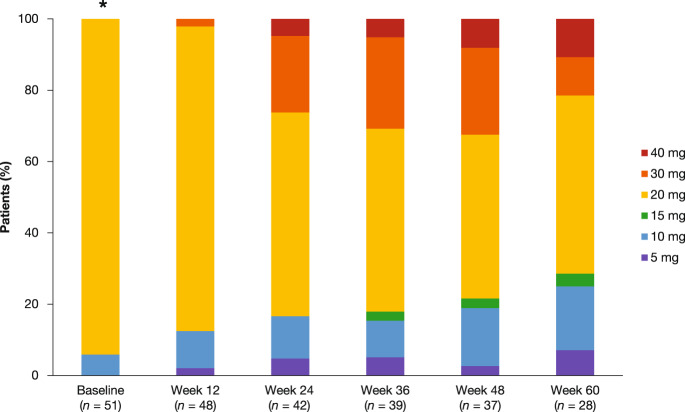
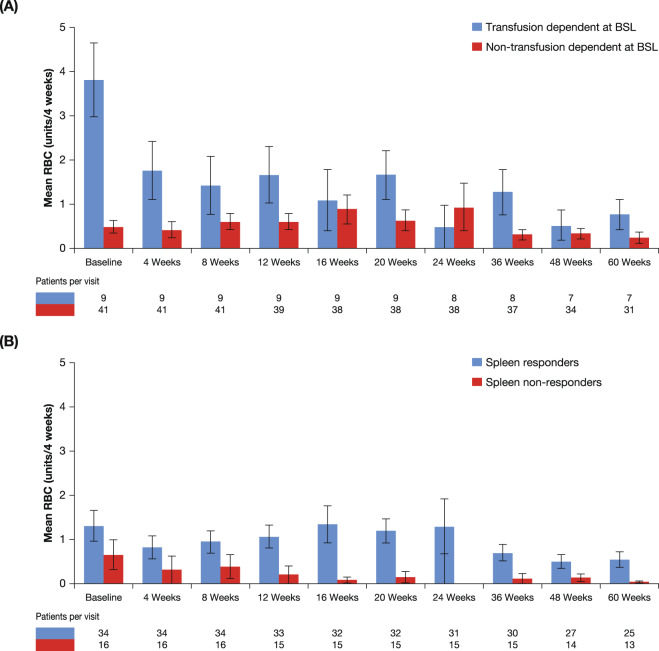
Anemia is a frequent manifestation of myelofibrosis (MF) and there is an unmet need for effective treatments in anemic MF patients. The REALISE phase 2 study (NCT02966353) evaluated the efficacy and safety of a novel ruxolitinib dosing strategy with a reduced starting dose with delayed up-titration in anemic MF patients. Fifty-one patients with primary MF (66.7%), post-essential thrombocythemia MF (21.6%), or post-polycythemia vera MF (11.8%) with palpable splenomegaly and hemoglobin <10 g/dl were included. Median age was 67 (45-88) years, 41.2% were female, and 18% were transfusion-dependent. Patients received 10 mg ruxolitinib b.i.d. for the first 12 weeks, then up-titrations of up to 25 mg b.i.d. were permitted, based on efficacy and platelet counts. Overall, 70% of patients achieved a ≥50% reduction in palpable spleen length at any time during the study. The most frequent adverse events leading to dose interruption/adjustment were thrombocytopenia (17.6%) and anemia (11.8%). Patients who had a dose increase had greater spleen size and higher white blood cell counts at baseline. Median hemoglobin levels remained stable and transfusion requirements did not increase compared with baseline. These results reinforce the notion that it is unnecessary to delay or withhold ruxolitinib because of co-existent or treatment-emergent anemia.
© 2021. The Author(s).
Conflict of interest statement
FC has served on speakers’ bureaus and advisory boards for Celgene and Novartis. DMR has received consultancy fees, honoraria, and research funding from Novartis, consultancy fees and honoraria from Bristol-Myers Squibb and Celgene, and research funding from Celgene. FPal has received speaker’s honoraria from Novartis. AMV has served on speakers’ bureaus for Gilead and Shire, and has served on the board of directors, speakers’ bureaus or advisory committees for and received research funding from Novartis. HG has received consultancy fees, honoraria, and research funding from, and served on speakers’ bureaus for AOP ORPHAN and Celgene, has received consultancy fees, honoraria, and research funding from Novartis, has received honoraria from and has served on speakers’ bureaus for Janssen Cilag. NK has received research funding from Fuso Pharmaceutical Industries and Wako Pure Chemical Industries, has received research funding from and has served on speakers’ bureaus for PharmaEssentia and Takeda, and has served on speakers’ bureaus for Novartis. LF has received consultancy fees from Pfizer, research funding from Constellation, Gilead, Incyte, and Promedior, and consultancy fees, honoraria, and research funding from Novartis. FPas has served on speakers’ bureaus for Novartis and Celgene/BMS. GG, IS, RT, and EZ are employees of Novartis. HKA-A has received consultancy fees, honoraria, and research funding from Novartis and Celgene, honoraria from Alexion, and consultancy fees and honoraria from Gilead. AR, AM, PZ, FM declare no conflicts of interest.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
