

Therapeutic trials in adult FSGS: lessons learned and the road forward
- PMID: 34017116
- PMCID: PMC8136112
- DOI: 10.1038/s41581-021-00427-1
Therapeutic trials in adult FSGS: lessons learned and the road forward
Abstract
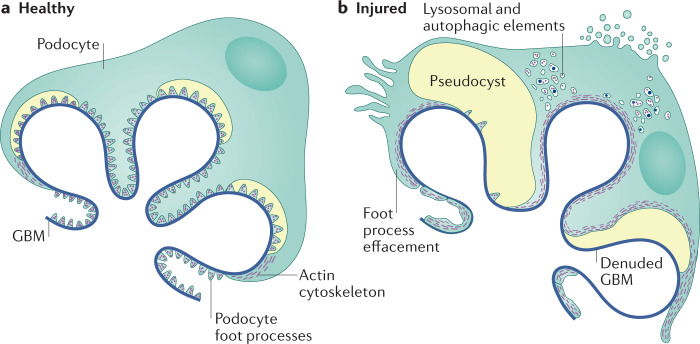
Focal segmental glomerulosclerosis (FSGS) is not a specific disease entity but a lesion that primarily targets the podocyte. In a broad sense, the causes of the lesion can be divided into those triggered by a presumed circulating permeability factor, those that occur secondary to a process that might originate outside the kidneys, those caused by a genetic mutation in a podocyte or glomerular basement membrane protein, and those that arise through an as yet unidentifiable process, seemingly unrelated to a circulating permeability factor. A careful attempt to correctly stratify patients with FSGS based on their clinical presentation and pathological findings on kidney biopsy is essential for sound treatment decisions in individual patients. However, it is also essential for the rational design of therapeutic trials in FSGS. Greater recognition of the pathophysiology underlying podocyte stress and damage in FSGS will increase the likelihood that the cause of an FSGS lesion is properly identified and enable stratification of patients in future interventional trials. Such efforts will facilitate the identification of effective therapeutic agents.
© 2021. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Velosa JA, Donadio JV, Jr, Holley KE. Focal sclerosing glomerulonephropathy: a clinicopathologic study. Mayo Clin. Proc. 1975;50:121–133. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
