

Mortality and Outcomes of Pediatric Tracheostomy Dependent Patients
- PMID: 34017809
- PMCID: PMC8129024
- DOI: 10.3389/fped.2021.661512
Mortality and Outcomes of Pediatric Tracheostomy Dependent Patients
Abstract
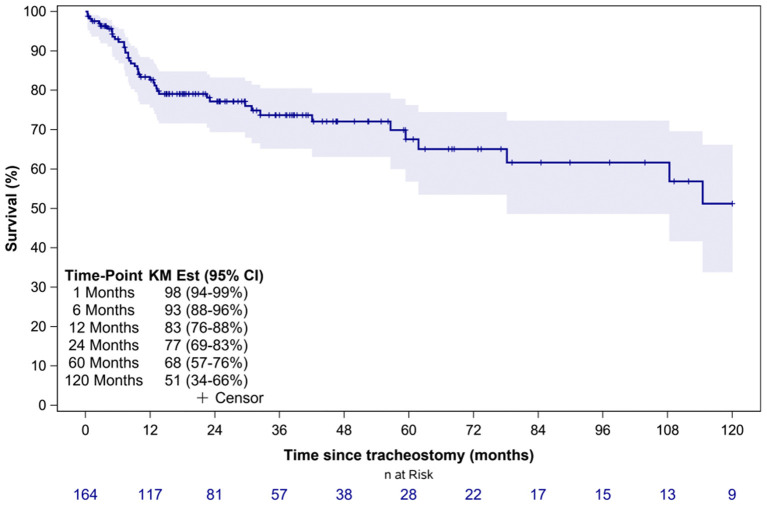
Objective: To describe clinical factors associated with mortality and causes of death in tracheostomy-dependent (TD) children. Methods: A retrospective study of patients with a new or established tracheostomy requiring hospitalization at a large tertiary children's hospital between 2009 and 2015 was conducted. Patient groups were developed based on indication for tracheostomy: pulmonary, anatomic/airway obstruction, and neurologic causes. The outcome measures were overall mortality rate, mortality risk factors, and causes of death. Results: A total of 187 patients were identified as TD with complete data available for 164 patients. Primary indications for tracheostomy included pulmonary (40%), anatomic/airway obstruction (36%), and neurologic (24%). The median age at tracheostomy and duration of follow up were 6.6 months (IQR 3.5-19.5 months) and 23.8 months (IQR 9.9-46.7 months), respectively. Overall, 45 (27%) patients died during the study period and the median time to death following tracheostomy was 9.8 months (IQR 6.1-29.7 months). Overall survival at 1- and 5-years following tracheostomy was 83% (95% CI: 76-88%) and 68% (95% CI: 57-76%), respectively. There was no significant difference in mortality based on indication for tracheostomy (p = 0.35), however pulmonary indication for tracheostomy was associated with a shorter time to death (HR: 1.9; 95% CI: 1.04-3.4; p = 0.04). Among the co-morbid medical conditions, children with seizure disorder had higher mortality (p = 0.04). Conclusion: In this study, TD children had a high mortality rate with no significant difference in mortality based on indication for tracheostomy. Pulmonary indication for tracheostomy was associated with a shorter time to death and neurologic indication was associated with lower decannulation rates.
Keywords: decannulation; mortality; outcome; pediatric; tracheostomy.
Copyright © 2021 Hebbar, Kasi, Vielkind, McCracken, Ivie, Prickett and Simon.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Keens TG, Kun SS, Ward SLD. Chronic respiratory failure. In: Shaffner DH, Nichols DG. editors. Rogers' Textbook of Pediatric Intensive Care, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; (2015). p. 794–807.
LinkOut - more resources
Full Text Sources
Other Literature Sources