

Prediction of COVID-19 Hospital Length of Stay and Risk of Death Using Artificial Intelligence-Based Modeling
- PMID: 34017839
- PMCID: PMC8129500
- DOI: 10.3389/fmed.2021.592336
Prediction of COVID-19 Hospital Length of Stay and Risk of Death Using Artificial Intelligence-Based Modeling
Abstract
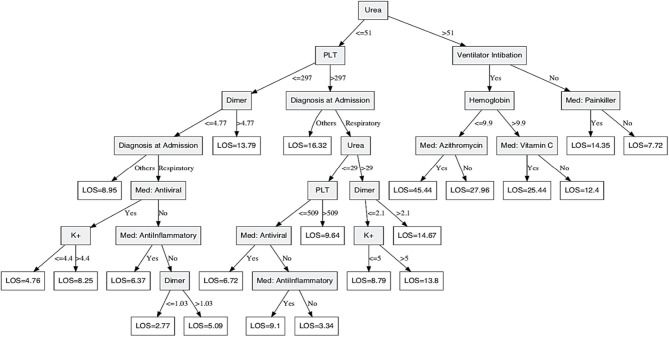
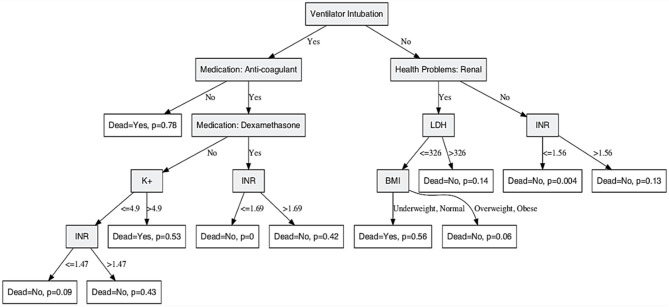
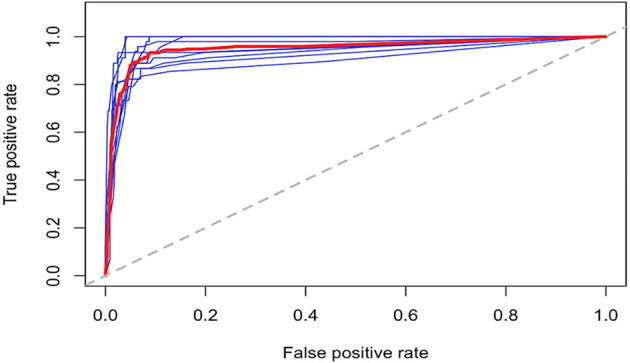
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a highly infectious virus with overwhelming demand on healthcare systems, which require advanced predictive analytics to strategize COVID-19 management in a more effective and efficient manner. We analyzed clinical data of 2017 COVID-19 cases reported in the Dubai health authority and developed predictive models to predict the patient's length of hospital stay and risk of death. A decision tree (DT) model to predict COVID-19 length of stay was developed based on patient clinical information. The model showed very good performance with a coefficient of determination R 2 of 49.8% and a median absolute deviation of 2.85 days. Furthermore, another DT-based model was constructed to predict COVID-19 risk of death. The model showed excellent performance with sensitivity and specificity of 96.5 and 87.8%, respectively, and overall prediction accuracy of 96%. Further validation using unsupervised learning methods showed similar separation patterns, and a receiver operator characteristic approach suggested stable and robust DT model performance. The results show that a high risk of death of 78.2% is indicated for intubated COVID-19 patients who have not used anticoagulant medications. Fortunately, intubated patients who are using anticoagulant and dexamethasone medications with an international normalized ratio of <1.69 have zero risk of death from COVID-19. In conclusion, we constructed artificial intelligence-based models to accurately predict the length of hospital stay and risk of death in COVID-19 cases. These smart models will arm physicians on the front line to enhance management strategies to save lives.
Keywords: COVID-19; artificial intelligence; length of stay; predictive analytics; risk of death.
Copyright © 2021 Mahboub, Bataineh, Alshraideh, Hamoudi, Salameh and Shamayleh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Pickering BW, Dong Y, Ahmed A, Giri J, Kilickaya O, Gupta A, et al. The implementation of clinician designed, human-centered electronic medical record viewer in the intensive care unit: a pilot step-wedge cluster randomized trial. Int J Med Inform. (2015) 84:299–307. 10.1016/j.ijmedinf.2015.01.017 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous