

Inpatient Frailty Assessment Is Feasible and Predicts Nonhome Discharge and Mortality in Decompensated Cirrhosis
- PMID: 34018303
- PMCID: PMC8809112
- DOI: 10.1002/lt.26100
Inpatient Frailty Assessment Is Feasible and Predicts Nonhome Discharge and Mortality in Decompensated Cirrhosis
Abstract
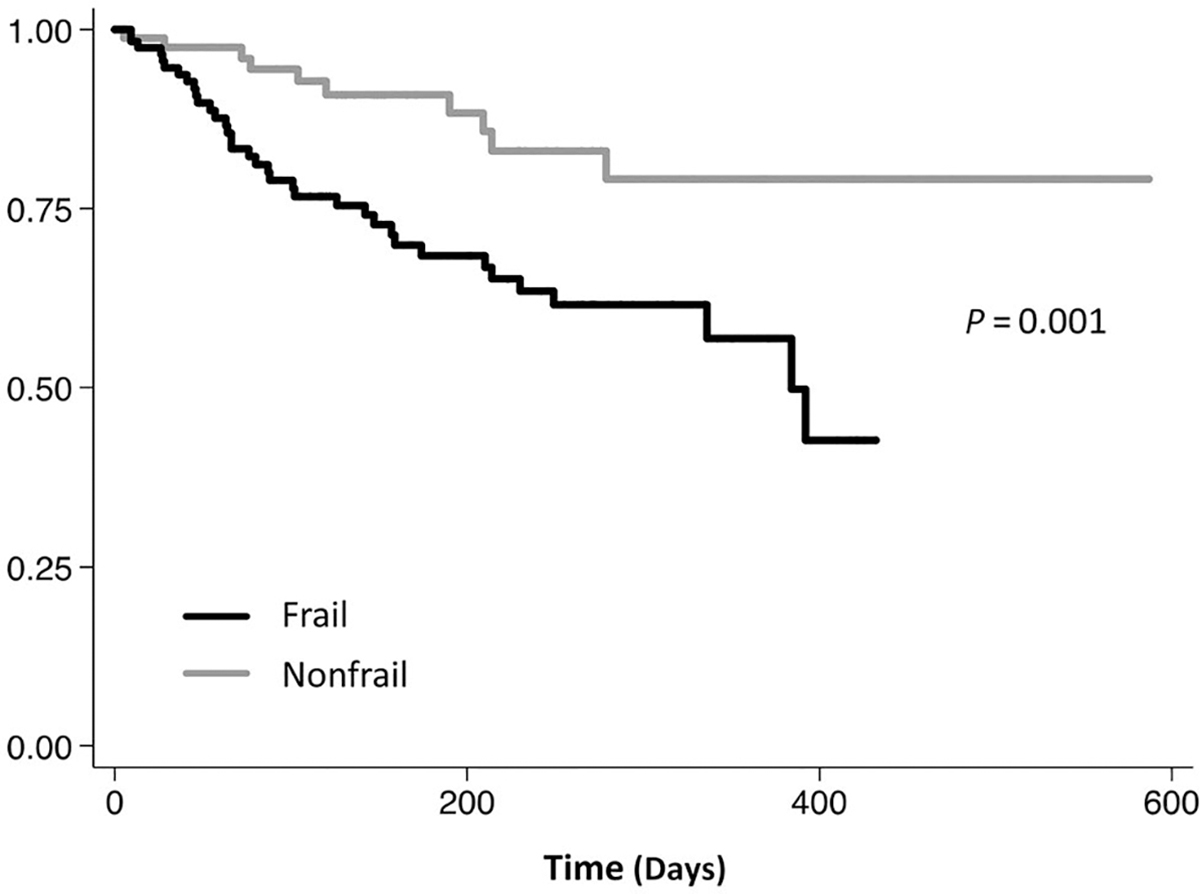
Objective inpatient frailty assessments in decompensated cirrhosis are understudied. We examined the feasibility of inpatient frailty measurements and associations with nonhome discharge, readmission, and all-cause mortality among patients admitted for cirrhosis complications. We conducted a prospective study at 3 liver transplantation (LT) centers. Frailty was assessed using the liver frailty index (LFI). Multivariable logistic and competing risk models evaluated associations between frailty and clinical outcomes. We included 211 patients with median MELD-Na score 21 (interquartile range [IQR],15-27); 96 (45%) were women, and 102 (48%) were on the LT waiting list. At a median follow-up of 8.3 months, 29 patients (14%) were nonhome discharged, 144 (68%) were readmitted, 70 (33%) underwent LT, and 44 (21%) died. A total of 124 patients (59%) were frail, with a median LFI of 4.71 (IQR, 4.07-5.54). Frail patients were older (mean, 59 versus 54 years) and more likely to have chronic kidney disease (40% versus 20%; P = 0.002) and coronary artery disease (17% versus 7%; P = 0.03). Frailty was associated with hospital-acquired infections (8% versus 1%; P = 0.02). In multivariable models, LFI was associated with nonhome discharge (odds ratio, 1.81 per 1-point increase; 95% confidence interval [CI], 1.14-2.86). Frailty (LFI≥4.5) was associated with all-cause mortality in models accounting for LT as competing risk (subhazard ratio [sHR], 2.4; 95% CI, 1.13-5.11); results were similar with LFI as a continuous variable (sHR, 1.62 per 1-point increase; 95% CI, 1.15-2.28). A brief, objective inpatient frailty assessment was feasible and predicted nonhome discharge and mortality in decompensated cirrhosis. Inpatient point-of-care frailty assessment prior to hospital discharge can be useful for risk stratification and targeted interventions to improve physical fitness and reduce adverse outcomes.
Copyright © 2021 by the American Association for the Study of Liver Diseases.
Figures




Comment in
-
Measuring the Toll of Acute Illness-Derived Frailty in Decompensated Cirrhosis.Liver Transpl. 2021 Dec;27(12):1701-1703. doi: 10.1002/lt.26249. Epub 2021 Aug 24. Liver Transpl. 2021. PMID: 34338440 No abstract available.
References
-
- Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001;56:M146–M156. - PubMed
-
- Tapper EB, Derstine B, Baki J, Su GL. Bedside measures of frailty and cognitive function correlate with sarcopenia in patients with cirrhosis. Dig Dis Sci 2019;64:3652–3659. - PubMed
-
- Duarte-Rojo A, Ruiz-Margain A, Montano-Loza AJ, Macias-Rodriguez RU, Ferrando A, Kim WR. Exercise and physical activity for patients with end-stage liver disease: Improving functional status and sarcopenia while on the transplant waiting list. Liver Transpl 2018;24:122–139. - PubMed
-
- Kulkarni SS, Chen H, Josbeno DA, Schmotzer A, Hughes C, Humar A, et al. Gait speed and grip strength are associated with dropping out of the liver transplant waiting list. Transplant Proc 2019;51:794–797. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
