

Secondary sclerosing cholangitis as cause of persistent jaundice in patients with severe COVID-19
- PMID: 34018314
- PMCID: PMC8242687
- DOI: 10.1111/liv.14971
Secondary sclerosing cholangitis as cause of persistent jaundice in patients with severe COVID-19
Abstract
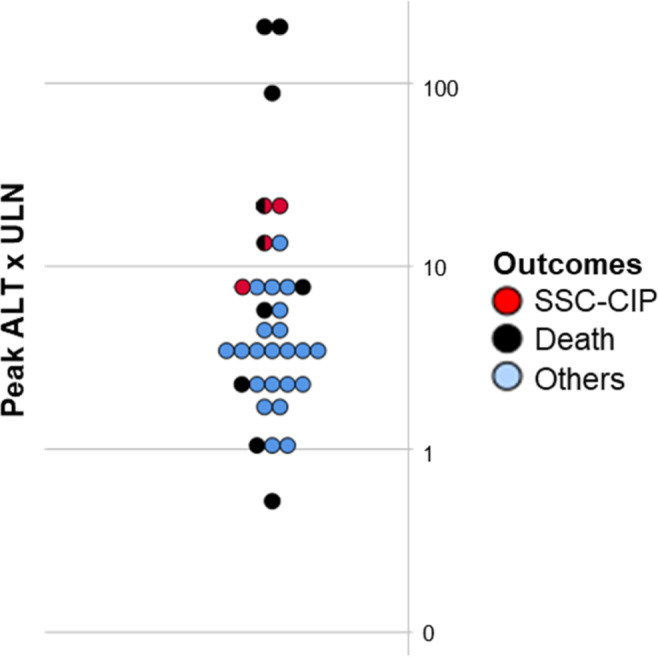
Background & aims: Little is known about cholestasis, including its most severe variant secondary sclerosing cholangitis (SSC), in critically ill patients with coronavirus disease 19 (COVID-19). In this study, we analysed the occurrence of cholestatic liver injury and SSC, including clinical, serological, radiological and histopathological findings.
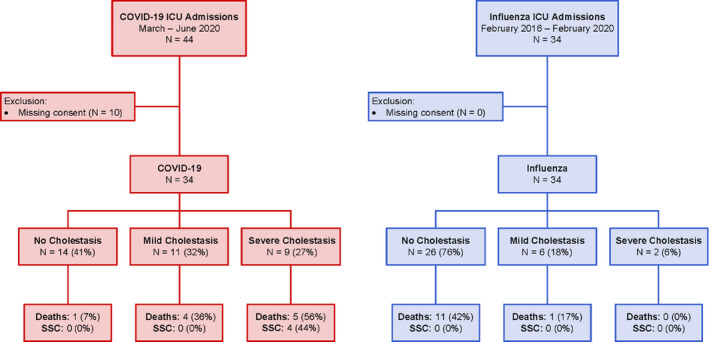
Methods: We conducted a retrospective single-centre analysis of all consecutive patients admitted to the intensive care unit (ICU) as a result of severe COVID-19 at the University Hospital Zurich to describe cholestatic injury in these patients. The findings were compared to a retrospective cohort of patients with severe influenza A.
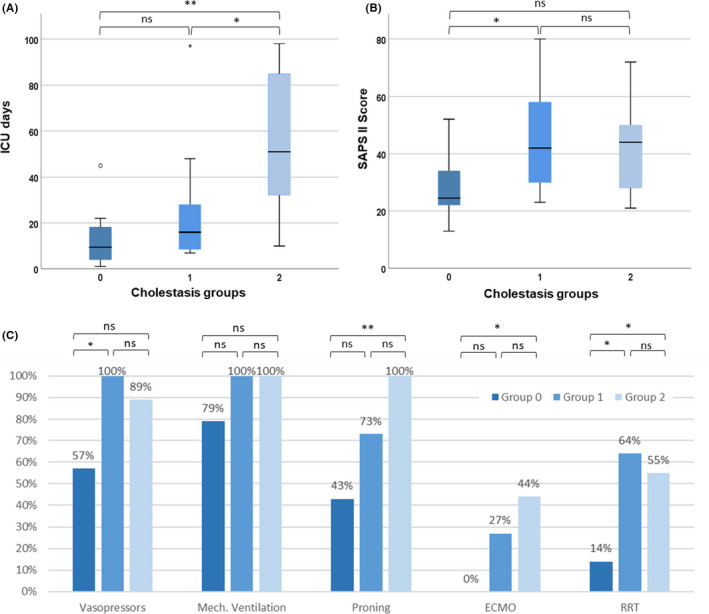
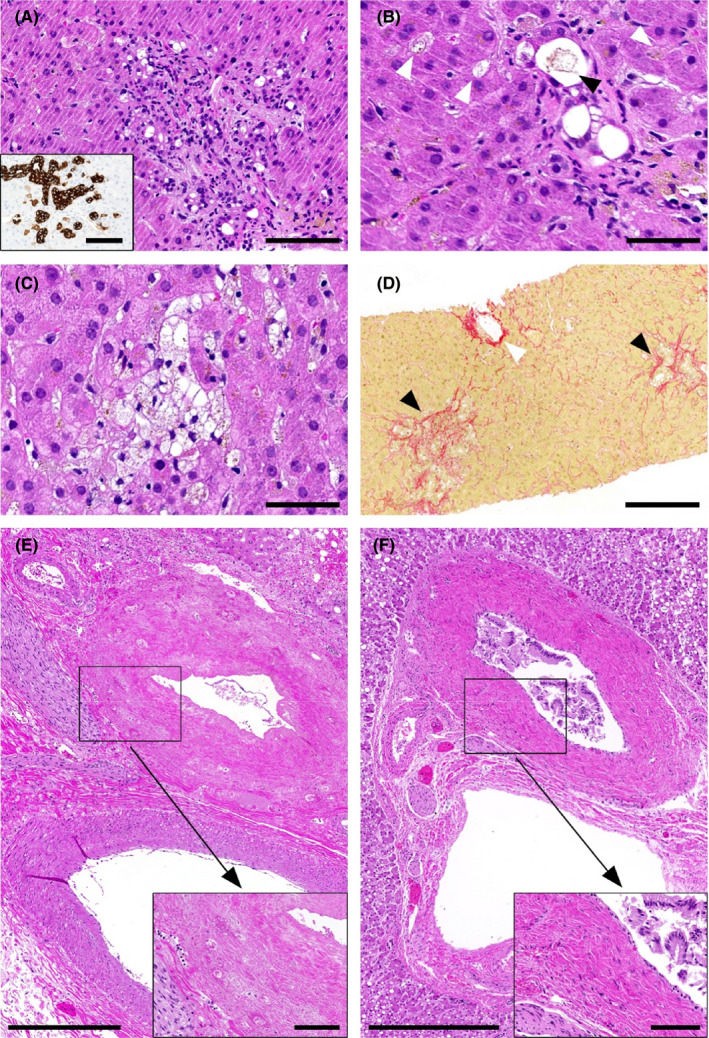
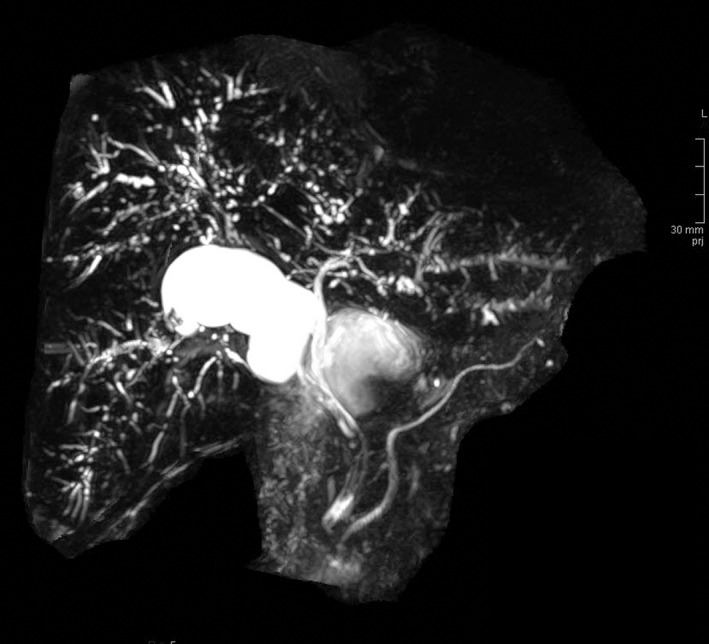
Results: A total of 34 patients with severe COVID-19 admitted to the ICU were included. Of these, 14 patients (41%) had no cholestasis (group 0), 11 patients (32%, group 1) developed mild and 9 patients (27%, group 2) severe cholestasis. Patients in group 2 had a more complicated disease course indicated by significantly longer ICU stay (median 51 days, IQR 25-86.5) than the other groups (group 0: median 9.5 days, IQR 3.8-18.3, P = .001; and group 1: median 16 days, IQR 8-30, P < .05 respectively). Four patients in group 2 developed SSC compared to none in the influenza A cohort. The available histopathological findings suggest an ischaemic damage to the perihilar bile ducts.
Conclusions: The development of SSC represents an important complication of critically ill COVID-19 patients and needs to be considered in the diagnostic work up in prolonged cholestasis. The occurrence of SSC is of interest in the ongoing pandemic since it is associated with considerable morbidity and mortality.
Keywords: Coronavirus disease 19 (COVID-19); cholestasis; liver injury; sclerosing cholangitis in critically ill patients; secondary sclerosing cholangitis; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
© 2021 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
BMo: none. BMü: has received speaking and/or consulting fees from Merck/MSD, AbbVie, Intercept, Astra, Bayer and Gilead and research support from Gilead. CJ: none. CG: none. CSR: none. DL: none. EMM: none. GB: none. KPB: none. MH: none. PDWG: none. SB: none.
Figures
References
-
- WHO . Coronavirus disease 2019 (COVID‐19) situation report. [Website]. https://www.who.int/publications/m/item/weekly‐epidemiological‐update‐‐‐...
-
- Lin T, Qu K, Xu X, et al. Sclerosing cholangitis in critically ill patients: an important and easily ignored problem based on a German experience. Front Med. 2014;8(1):118‐126. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
