

Postinfusion monitoring costs by site of care for patients with relapsed/refractory large B-cell lymphoma receiving third- or later-line treatment with lisocabtagene maraleucel in the TRANSCEND NHL 001 and OUTREACH trials
- PMID: 34018458
- PMCID: PMC9400457
- DOI: 10.1080/10428194.2021.1910686
Postinfusion monitoring costs by site of care for patients with relapsed/refractory large B-cell lymphoma receiving third- or later-line treatment with lisocabtagene maraleucel in the TRANSCEND NHL 001 and OUTREACH trials
Abstract
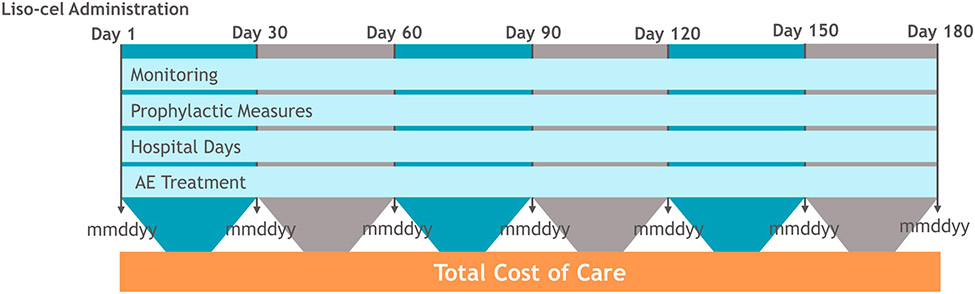
This retrospective study estimated postinfusion health care resource utilization (HCRU) by site of care among 303 patients with relapsed/refractory large B-cell lymphoma who received third- or later-line treatment with lisocabtagene maraleucel (liso-cel) in the TRANSCEND NHL 001 and OUTREACH trials. Inpatients (n = 256) had higher rates of hospitalization versus outpatients (n = 47; >99% vs 62%), by definition, and higher rates of tocilizumab use for cytokine release syndrome and/or neurological events (22% vs 9%). Rates of intensive care unit admission, corticosteroid use, vasopressor use, hemodialysis, and intubation were generally low and similar between groups. Median (range) total hospital length of stay was 15 (0-88) days (inpatients) and 4 (0-77) days (outpatients). Over 6 months, estimated mean postinfusion cost of care was $89,535 (inpatients) and $36,702 (outpatients). Most costs were incurred in the first month post infusion (inpatients, $50,369 [56%]; outpatients, $19,837 [54%]). Lower overall HCRU was observed with outpatient postinfusion monitoring.
Keywords: CAR T cell therapy; cost; economic burden; inpatient and/or outpatient monitoring; lisocabtagene maraleucel; resource utilization.
Conflict of interest statement
Disclosure of interest
M. Lia Palomba reports personal fees and other from Merck, personal fees from Novartis, personal fees and other from Pharmacyclics, personal fees and other from Kite, personal fees from BeiGene, outside the submitted work; Dr. Palomba has intellectual property interests (by virtue of immediate family member interests) related to CARs (Chimeric Antigen Receptors) and TCRs (T cell Receptors) that Memorial Sloan Kettering Cancer Center (MSK) has licensed to Juno Therapeutics, a Bristol-Myers Squibb Company. Monika P. Jun, Scott Keating, James Lymp, and Corey Pelletier are employees of Bristol Myers Squibb and may hold stock in Bristol Myers Squibb. November McGarvey, Matthew Gitlin, and Andy Nguyen are employees of BluePath Solutions, which received funding from Bristol Myers Squibb, to conduct the analyses. John E. Godwin reports no conflict of interest.
Figures

References
-
- US Cancer Statistics Working Group. US Cancer Statistics Data Visualizations Tool, based on November 2018 submission data (1999-2016) [Internet]. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2019. [cited 2020 Oct 6]. Available from: https://gis.cdc.gov/Cancer/USCS/DataViz.html
-
- Armitage JO, Weisenburger DD. New approach to classifying non-Hodgkin's lymphomas: clinical features of the major histologic subtypes. Non-Hodgkin's Lymphoma Classification Project. J Clin Oncol. 1998;16(8):2780–2795. - PubMed
-
- A clinical evaluation of the International Lymphoma Study Group classification of non-Hodgkin's lymphoma. The Non-Hodgkin's Lymphoma Classification Project. Blood. 1997;89(11):3909–3918. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources