

Factors Associated With Use of an Online Telemedicine Service to Access Self-managed Medical Abortion in the US
- PMID: 34019085
- PMCID: PMC8140373
- DOI: 10.1001/jamanetworkopen.2021.11852
Factors Associated With Use of an Online Telemedicine Service to Access Self-managed Medical Abortion in the US
Abstract
Importance: People in the US have been seeking self-managed abortions outside the formal health care system using medications obtained through online telemedicine. However, little is known about this practice, including potential motivating factors.
Objective: To examine individual reasons for accessing medication abortion through an online telemedicine service as well as associations between state- and county-level factors and the rate of requests.
Design, setting, and participants: This population-based cross-sectional study examined all requests for self-managed medication abortion through an online consultation form available from Aid Access, a telemedicine service in the US, between March 20, 2018, and March 20, 2020.
Main outcomes and measures: Individual-level reasons for accessing the telemedicine service were examined as well as the rate of requests per 100 000 women of reproductive age by state. Zip code data provided by individuals making requests were used to examine county-level factors hypothesized to be associated with increased demand for self-managed abortion: distance to a clinic (calculated using location data for US abortion clinics) and the population proportion identifying as a member of a racial/ethnic minority group, living below the federal poverty level, and having broadband internet access (calculated using census data).
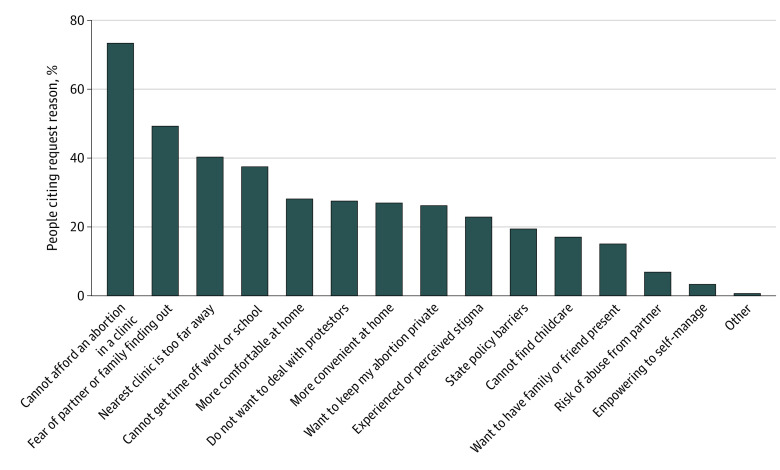
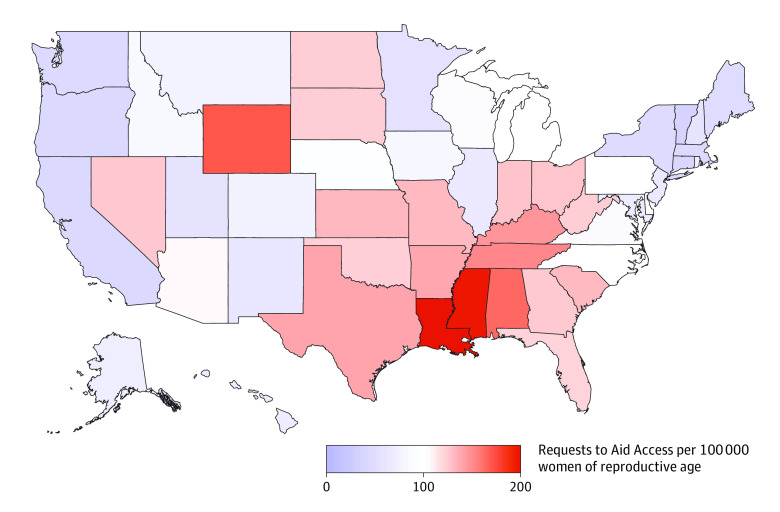
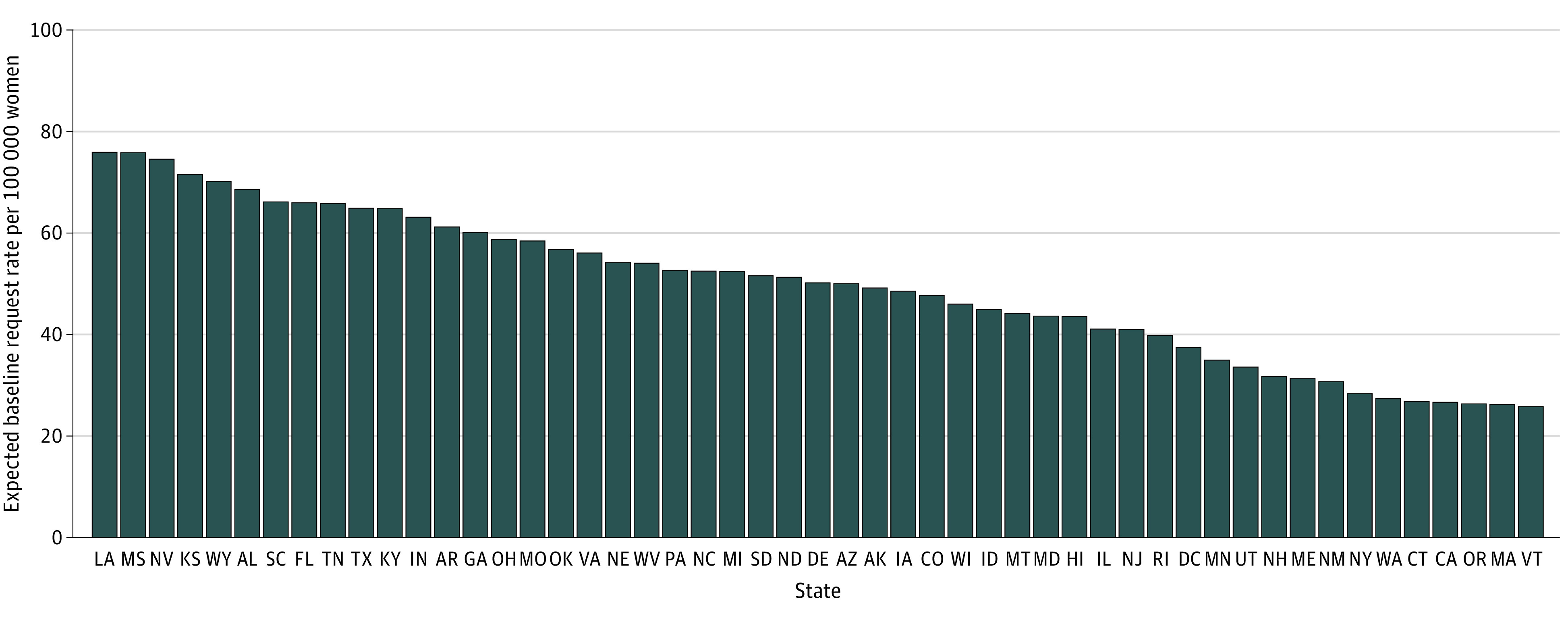
Results: During the 2-year study period, 57 506 individuals in 2458 counties in 50 states requested self-managed medication abortion; 52.1% were aged 20 to 29 years (mean [SD] age, 25.9 [6.7] years), 50.0% had children, and 99.9% were 10 weeks' pregnant or less. The most common reasons cited by individuals making requests were the inability to afford in-clinic care (73.5%), privacy (49.3%), and clinic distance (40.4%). States with the highest rate of requests were Louisiana (202.7 per 100 000 women) and Mississippi (199.9 per 100 000 women). At the county level, an increase of 1 SD (47 miles) in distance to the nearest clinic was significantly associated with a 41% increase in requests (incidence rate ratio, 1.41; 95% CI, 1.31-1.51; P < .001), and a 10% increase in the population living below the federal poverty level was significantly associated with a 20% increase in requests (incidence rate ratio, 1.20; 95% CI, 1.13-1.28; P < .001).
Conclusions and relevance: In this cross-sectional study, clinic access barriers were the most commonly cited reason for requesting self-managed medication abortion using an online telemedicine service. At the county level, distance to an abortion clinic and living below the federal poverty level were associated with a higher rate of requests. State and federal legislation could address these access barriers.
Conflict of interest statement
Figures
References
-
- World Health Organization Guidelines . WHO recommendations on self-care interventions: self-management of medical abortion. 25 June 2020. Accessed January 12, 2021. https://www.who.int/publications/i/item/WHO-SRH-20-11
-
- Nash E, Donovan MK. Ensuring access to abortion at the state level: selected examples and lessons. Guttmacher Policy Review. 2019;22. March 31, 2021. https://www.guttmacher.org/gpr/2019/01/ensuring-access-abortion-state-le...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
