

Adherence at 2 years with distribution of essential medicines at no charge: The CLEAN Meds randomized clinical trial
- PMID: 34019540
- PMCID: PMC8139488
- DOI: 10.1371/journal.pmed.1003590
Adherence at 2 years with distribution of essential medicines at no charge: The CLEAN Meds randomized clinical trial
Abstract
Background: Adherence to medicines is low for a variety of reasons, including the cost borne by patients. Some jurisdictions publicly fund medicines for the general population, but many jurisdictions do not, and such policies are contentious. To our knowledge, no trials studying free access to a wide range of medicines have been conducted.
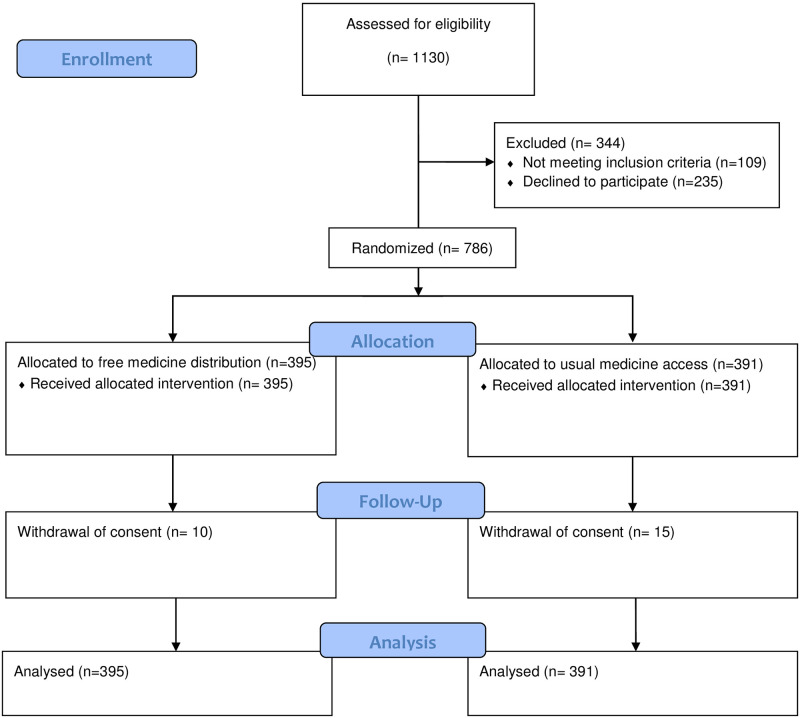
Methods and findings: We randomly assigned 786 primary care patients who reported not taking medicines due to cost between June 1, 2016 and April 28, 2017 to either free distribution of essential medicines (n = 395) or to usual medicine access (n = 391). The trial was conducted in Ontario, Canada, where hospital care and physician services are publicly funded for the general population but medicines are not. The trial population was mostly female (56%), younger than 65 years (83%), white (66%), and had a low income from wages as the primary source (56%). The primary outcome was medicine adherence after 2 years. Secondary outcomes included control of diabetes, blood pressure, and low-density lipoprotein (LDL) cholesterol in patients taking relevant treatments and healthcare costs over 2 years. Adherence to all appropriate prescribed medicines was 38.7% in the free distribution group and 28.6% in the usual access group after 2 years (absolute difference 10.1%; 95% confidence interval (CI) 3.3 to 16.9, p = 0.004). There were no statistically significant differences in control of diabetes (hemoglobin A1c 0.27; 95% CI -0.25 to 0.79, p = 0.302), systolic blood pressure (-3.9; 95% CI -9.9 to 2.2, p = 0.210), or LDL cholesterol (0.26; 95% CI -0.08 to 0.60, p = 0.130) based on available data. Total healthcare costs over 2 years were lower with free distribution (difference in median CAN$1,117; 95% CI CAN$445 to CAN$1,778, p = 0.006). In the free distribution group, 51 participants experienced a serious adverse event, while 68 participants in the usual access group experienced a serious adverse event (p = 0.091). Participants were not blinded, and some outcomes depended on participant reports.
Conclusions: In this study, we observed that free distribution of essential medicines to patients with cost-related nonadherence substantially increased adherence, did not affect surrogate health outcomes, and reduced total healthcare costs over 2 years.
Trial registration: ClinicalTrials.gov NCT02744963.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: PJ serves as unpaid member of steering group or executive committee of trials funded by Abbott Vascular, Astra Zeneca, Biotronik, Biosensors, St. Jude Medical, Terumo and The Medicines Company, has received research grants to the institution from Appili Therapeutics, Astra Zeneca, Biotronik, Biosensors International, Eli Lilly, The Medicines Company, and honoraria to the institution for participation in advisory boards and/or consulting from Amgen, Ava and Fresenius, but has not received personal payments by any pharmaceutical company or device manufacturer. MRL has consulted for Health Canada, the Hospital Employees’ Union, the Conference Board of Canada, and provided expert witness testimony for the Attorney General of Canada. MM has received honoraria for serving as a member of an Advisory Board for NovoNordisk.
References
-
- Elliott RA, Boyd MJ, Tanajewski L, Barber N, Gkountouras G, Avery AJ, et al.. ‘New Medicine Service’: supporting adherence in people starting a new medication for a long-term condition: 26-week follow-up of a pragmatic randomised controlled trial. BMJ Qual Saf. 2019:bmjqs-2018-009177. 10.1136/bmjqs-2018-009177 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
