

Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers - A multicentre cross-sectional study
- PMID: 34020033
- PMCID: PMC8131187
- DOI: 10.1016/j.cmi.2021.05.014
Non-occupational and occupational factors associated with specific SARS-CoV-2 antibodies among hospital workers - A multicentre cross-sectional study
Abstract
Objectives: Protecting healthcare workers (HCWs) from coronavirus disease-19 (COVID-19) is critical to preserve the functioning of healthcare systems. We therefore assessed seroprevalence and identified risk factors for severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) seropositivity in this population.
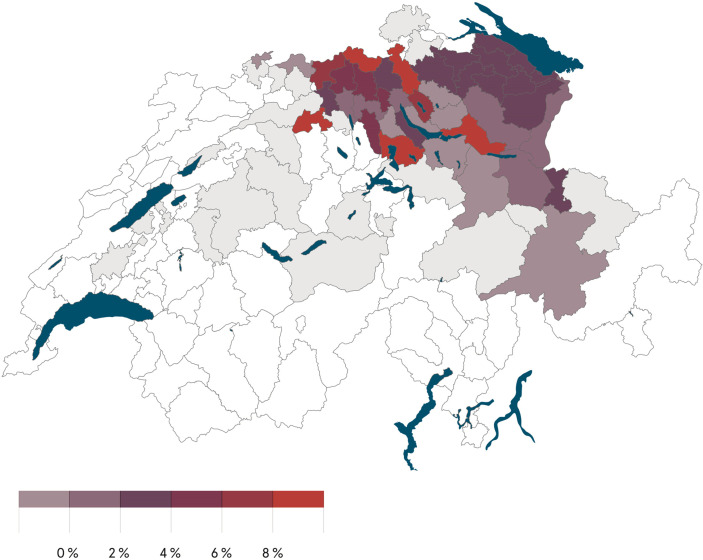
Methods: Between 22 June 22 and 15 August 2020, HCWs from institutions in northern/eastern Switzerland were screened for SARS-CoV-2 antibodies. We recorded baseline characteristics, non-occupational and occupational risk factors. We used pairwise tests of associations and multivariable logistic regression to identify factors associated with seropositivity.
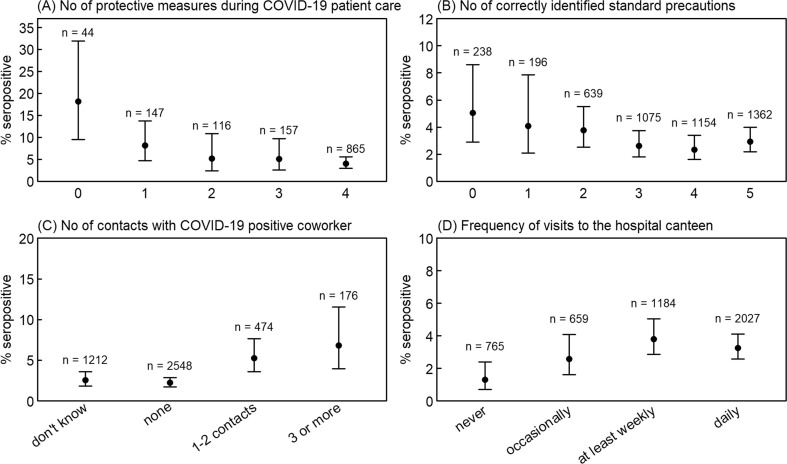
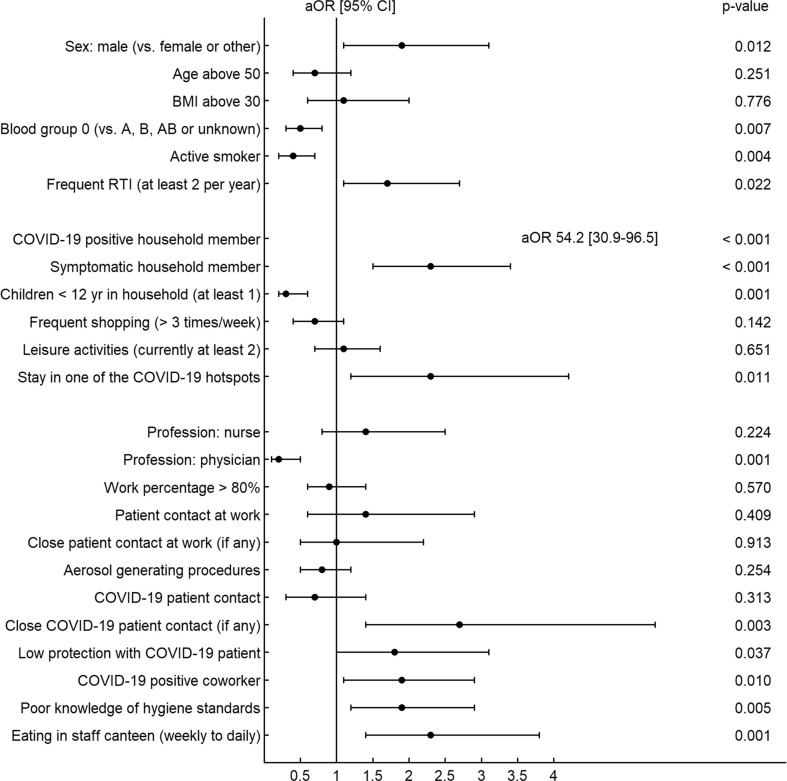
Results: Among 4664 HCWs from 23 healthcare facilities, 139 (3%) were seropositive. Non-occupational exposures independently associated with seropositivity were contact with a COVID-19-positive household (adjusted OR 59, 95% CI 33-106), stay in a COVID-19 hotspot (aOR 2.3, 95% CI 1.2-4.2) and male sex (aOR 1.9, 95% CI 1.1-3.1). Blood group 0 vs. non-0 (aOR 0.5, 95% CI 0.3-0.8), active smoking (aOR 0.4, 95% CI 0.2-0.7), living with children <12 years (aOR 0.3, 95% CI 0.2-0.6) and being a physician (aOR 0.2, 95% CI 0.1-0.5) were associated with decreased risk. Other occupational risk factors were close contact to COVID-19 patients (aOR 2.7, 95% CI 1.4-5.4), exposure to COVID-19-positive co-workers (aOR 1.9, 95% CI 1.1-2.9), poor knowledge of standard hygiene precautions (aOR 1.9, 95% CI 1.2-2.9) and frequent visits to the hospital canteen (aOR 2.3, 95% CI 1.4-3.8).
Discussion: Living with COVID-19-positive households showed the strongest association with SARS-CoV-2 seropositivity. We identified several potentially modifiable work-related risk factors, which might allow mitigation of the COVID-19 risk among HCWs. The lower risk among those living with children, even after correction for multiple confounders, is remarkable and merits further study.
Keywords: COVID-19; Healthcare workers; Risk factors; Seroprevalence; Switzerland.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- COVID-19 map Johns hopkins coronavirus resource center. https://coronavirus.jhu.edu/map.html Available at:
-
- Swiss Federal Office of Public Health Current situation in Switzerland -Daily report. https://www.covid19.admin.ch/en/overview?ovTime=total Available at:
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
